For Feb/Mar 2024, we are looking at a recently released laser machine to perform direct SLT – selective laser trabeculoplasty (DSLT). Although SLT is well known, DSLT is sufficiently novel that a brief description is a good place to start.
The ‘direct’ descriptor references the absence of a handheld contact lens in the treatment process. The laser is applied to the trabecular meshwork directly through the peripheral cornea (Figure 1). Unlike SLT, no manual shot-by-shot targeting is needed. In fact, no manual targeting is needed at all. The device is able to identify and track the limbus, then deliver the whole laser sequence (typically 120 shots over 360 degrees) over a few seconds. The main benefit to this technology is a significant increase in the number of patients that can be treated per unit time.
This is particularly relevant as SLT is now established as recommended first line treatment by National Institute for Clinical Excellence (NICE) and other standard-setting bodies. If the technology can deliver on these remarkable promises, it stands to significantly shake up the established doctrine and SLT device market.
Marketing brochures and trade show talks, although helpful, may not convey the whole picture. In agreeing to review the BELKIN Vision Eagle laser, I wanted to wait until I was able to test it myself. As a glaucoma consultant performing frequent SLT, I was already interested in evaluating a unit. That demo is now complete and we have used the laser to treat 13 eyes. We have also waited until first follow-up, at four weeks, before sharing our first impressions here.
Experience
It is important to understand that the first-hand experience I describe below is based on a single morning treatment session. More nuanced opinions would likely occur with greater use, so do bear that limitation in mind. That being said, I will start by broadly considering the two parts of the treatment – the pre-treatment experience (primarily for the patient) and then the treatment experience (for both the patient but also the clinician).

The main aspect of the pre-treatment to be aware of is the speculum. BELKIN Vision provides a speculum for each treatment, as part of the procedure pack. Using one is critical as the device needs to see the full 360 degrees of the cornea or it will not be able to lock and track the eye. Sometimes the provided speculum is a little too narrow, so the trainers propose the operator stretch the wire a little, to increase the pull of the speculum. In all the seven patients I treated, the speculum was consistently the only uncomfortable part of the experience. Two conclusions fall from this – have an eye speculum in place is not pleasant but the laser is not particularly uncomfortable. Sharing this fact with the patient, that the ‘clip’ will be the worst bit, and the laser trivial by comparison, is both helpful and true.
The only other part of the preparation that is noteworthy is situating the patient on the machine and aligning it. We decided, based on experience offered by our trainer, to encourage the patients to stand against the device, once prepared. Our seven patients were treated this way, and it did feel preferable. It certainly simplifies interfacing the machine with larger patients as you avoid the torso and chest being bunched up in front of them. Once a user is familiar with the touch screen interface and platform control stick, the setup of the device can be completed in less than a minute in most cases. The laser platform is heavy and does need to be moved with a manual stick. This does take a bit of force but is not a problem.
Once setup is complete, the unit has active tracking of the eye, meaning it can adapt to eye movements and stop treating if any movements are too large. The treatment itself is as short as promised. In no more than two or three seconds, the device applies 120 shots of laser to the meshwork via the peripheral corneal. The patients do feel some discomfort during the treatment, but it appears minimal and also clearly brief. A small amount of subconjunctival haemorrhage can occur. I saw a trivial amount in only one of our treated patients. One individual did pull away because of the surprise when the treatment started, but the unit stopped treating as designed. Once they were repositioned, we were able to easily complete the treatment from the point that it stopped. We had to resort to traditional SLT treatment for one eye of one of the seven patients as significant corneal arcus prevented the device locking onto the limbus.
I understand that a software update is in development that would allow the user to manually override, forcing a lock, and thus allowing automated treatment. A total of 13 eyes were treated in the session, as one of the eight patients did not attend.
After the treatment, a drop of iopidine was instilled and pressure re-tested one hour later. We had a pressure spike in one of the seven patients (from 24T22 to 27T30), which is comparable with traditional SLT. No analgesia or postoperative drops were provided to any of the patients treated. Many sites performing DSLT and SLT do provide ketorolac for a few days, but we have stopped this of late.
Outcomes and published data
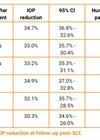
One of the patients did not attend the planned post-op appointment, providing us with results for 11 eyes. Of those, all eyes had a reduction in pressure (ranging from 10–56%) with an average of 28%. Again, these are comparable with traditional SLT. None of the patients reported any difficulties in the postoperative period and none of them needed to use analgesia. An randomised control trial (RCT) has been performed (‘GLAUrious’ study), comparing DSLT to SLT and is due to be published in early 2024. At present there is 12 months of data confirming non-inferiority of DSLT over SLT.
Impression
From the experience of using this device, it does appear to live up to the promises given. This hands-on experience, and short-term follow-up, confirms extremely fast, safe and effective treatment, comparable to SLT. The slowest part of the treatment becomes the informed consent. If this were, as some do, done outside of the clinic room by video, the BELKIN Vision Eagle could treat three times as many eyes as a traditional laser in a single session. We, in our eye unit, were sufficiently impressed that we are putting together a business case with the aim of procuring a device for regular use.
Cost and availability
Medical lasers are most often purchased outright, with the owner then able to use the laser as much or as little as desired, for no additional cost. The BELKIN unit is marketed more like phaco machines (or razor blades), where a ‘procedure pack’ needs to be purchased for each treatment. The advantage of this pricing model is a zero cost for the device, as long as 625 treatment packs are purchased each year, for three years. A set of 50 procedure packs consists of appropriate speculums and a QR code to activate the treatment licences. The treatment credits do not expire, allowing a unit to purchase the 1875 treatments, but take more than three years to use them. The device can also be purchased outright for £43,500 + VAT. Treatment credits are still purchased in the same way, at the same price of £66 + VAT per treated eye. The laser is guaranteed for two years in the UK, with a £3500 / year service contract needed thereafter.
At the time of writing, the device is available and fully licensed in the UK, Italy, Germany, Israel, Spain and Poland. In the UK, Carleton Optical is the supplier. (www.carletonltd.com)
✓ Shockingly fast when compared to traditional SLT.
✓ High build quality, polished and pleasant user interface.
✓ Appears equivalent to traditional SLT in safety, efficacy and likely repeatability.
? Inexpensive initially, but per treatment pricing will add up over time.
✓ High throughput likely to be an SLT market game changer.
The author has no proprietary or financial interests in the products discussed.
COMMENTS ARE WELCOME