Sickle cell disease or disorder (SCD) is one of the most neglected health conditions in the world. A strong hypothesis is that this is because SCD affects people of African, Caribbean and other Global Majority communities and has received disproportionately less focus, research and progress [1-3].
Sickle cell disease is a multisystem condition associated with chronic organ complications that increase with age (Figure 1) [4]. The systemic neglect of SCD extends to ocular complications, particularly sickle cell retinopathy (SCR), which remains under recognised and under researched despite its sight-threatening potential in people of working age [5]. Vision loss is just one of many devastating outcomes of this complex disorder.
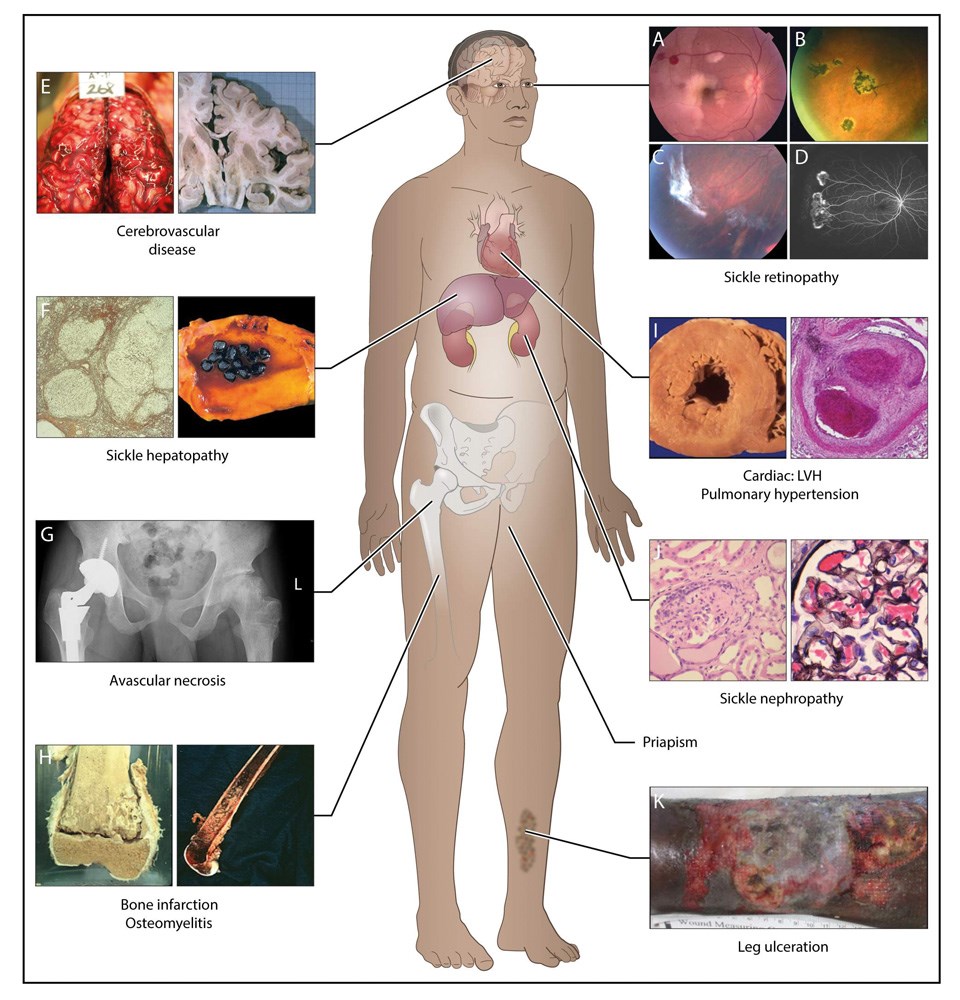
Figure 1: Complications commonly encountered in the older adult with SCD. This image highlights the multiorgan association of the condition. Reproduced with permission from Thein SL, Howard J. Blood. 2018;132(17):1750–60.
The Sickle Cell Retinopathy Network (SCR.net) is a global, multidisciplinary, not for profit organisation uniting ophthalmologists, haematologists, researchers and policymakers from countries where SCD is prevalent [6]. It is dedicated to conducting equitable multicentre research and developing evidence-based screening and management protocols to reduce vision threatening complications across all sickle cell genotypes.
The ethos of the SCR.net is an extremely bold ambition, which is to reverse the traditional flow of medical knowledge from the global north and instead centre the expertise and leadership of those closest to the burden of disease from the global south. Our vision is to reduce preventable blindness from SCR in all sickle cell genotypes by building consensus driven, evidence-based screening and treatment guidelines that are contextually relevant and globally inclusive [6].
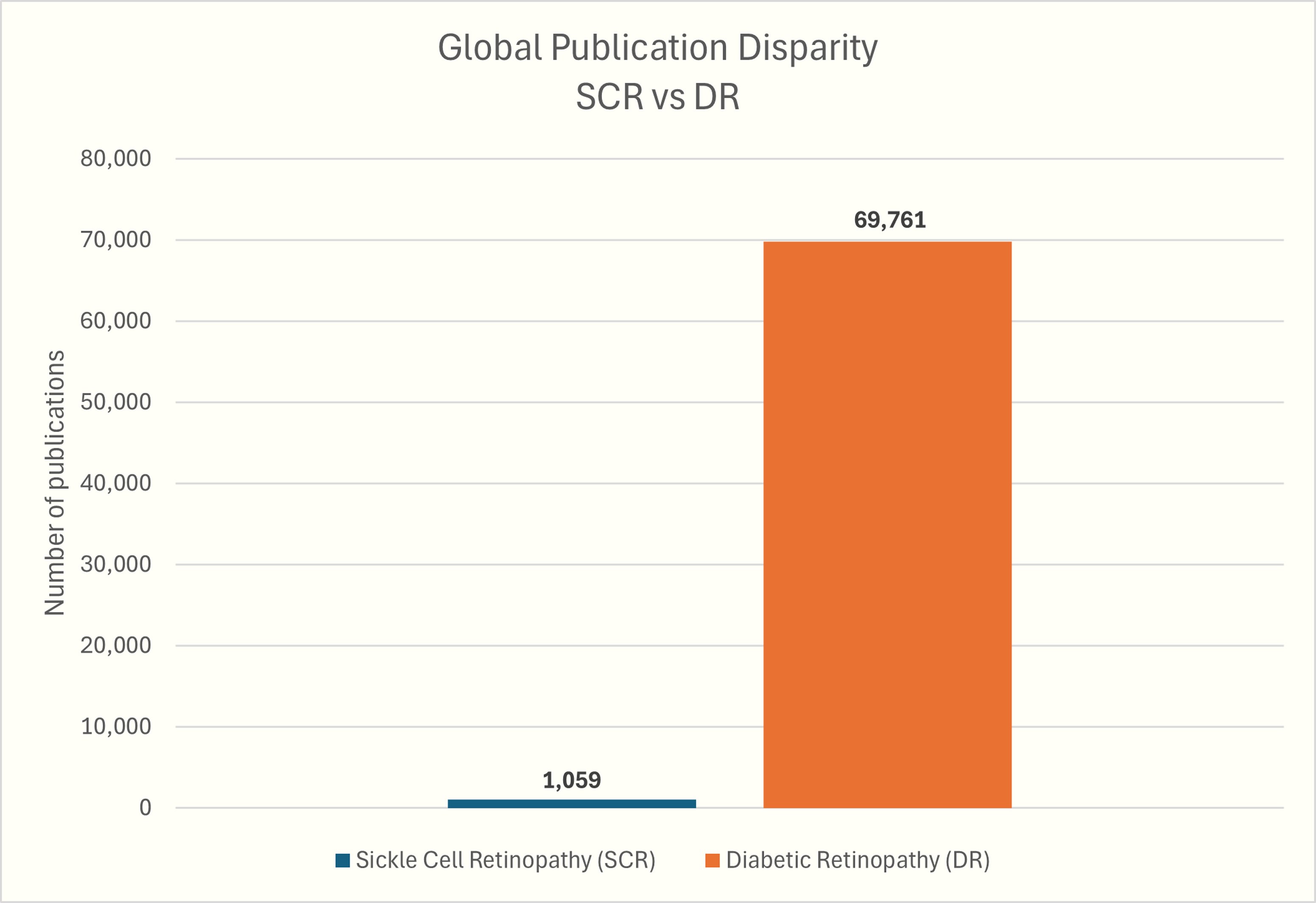
Figure 2: Bar chart showing the global publication disparity between DR and SCR over the past eight decades. Diabetic retinopathy has received nearly 70 times more research attention than SCR, despite comparable sight-threatening potential. Adapted with permission from Prof Nicholas Kassembaum [7].
Since its inception, SCR.net has identified several critical gaps. First, there are no globally accepted guidelines for the screening and management of SCR [5]. Second, research output on SCR lags dramatically behind more well-known retinal vascular diseases such as diabetic retinopathy (DR), despite similar sight-threatening potential. Our first consortium paper was a bibliometric analysis which identified just over 1000 global publications on SCR compared to nearly 70,000 on DR over the past eight decades (Figure 2) [8]. Most SCR studies originate from high-income countries, with minimal contributions from African or Caribbean nations, which are the regions where SCD is most prevalent (Figure 3).
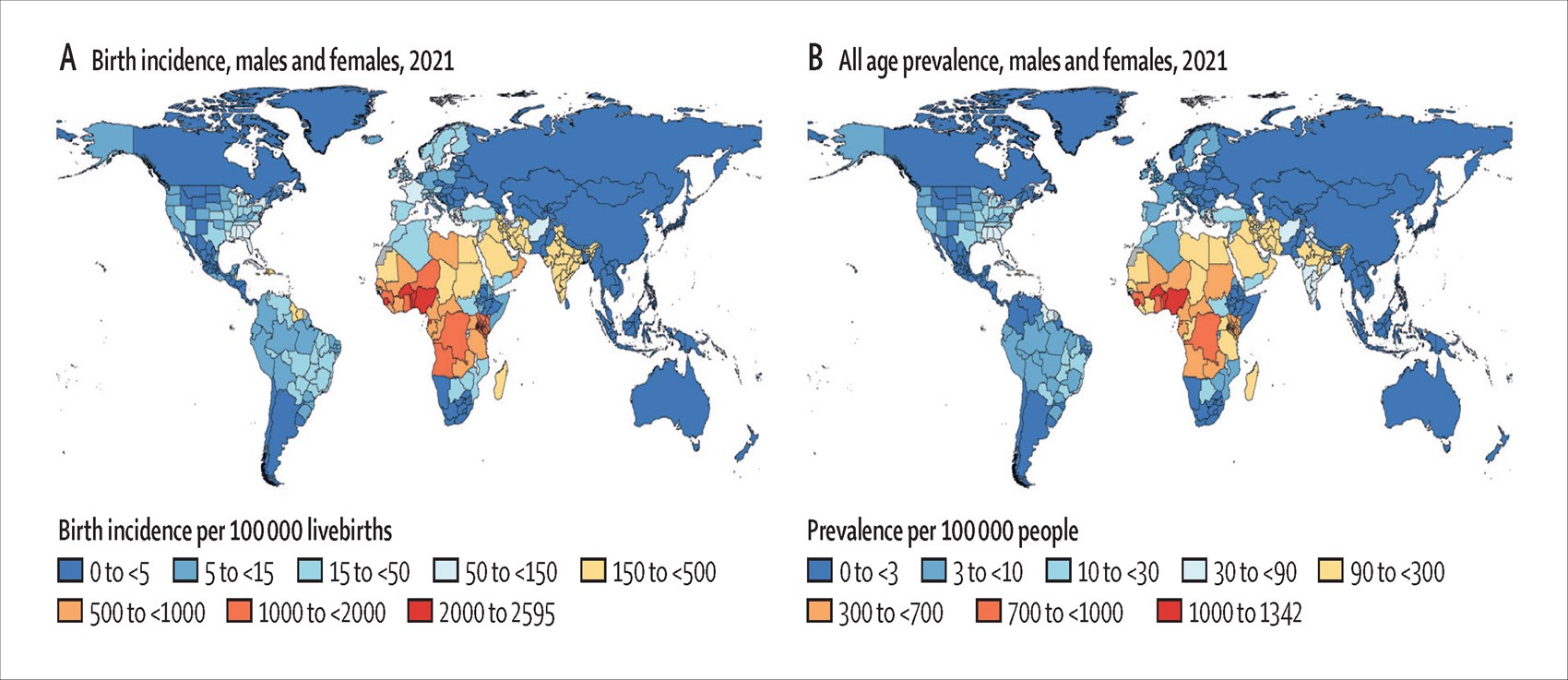
Figure 3: Global incidence and prevalence of SCD. Regions with the highest burden are in sub-Saharan Africa, South Asia, the Caribbean and Middle East. Adapted with permission from Prof Nicholas Kassebaum [7].
To redress this imbalance, SCR.net is leading a multi-round Delphi process to co-produce international consensus guidelines for SCR. This modified Delphi study engages a diverse panel from across the global south and north, including ophthalmologists, haematologists, patients, caregivers and public health policymakers. The study aims to build agreement on:
- Referral thresholds and integration into broader sickle cell care
- Who should be screened (including SCD genotypes and age thresholds)
- How frequently and with what modalities (e.g. ultra-widefield field photography and OCT)
- When and how to treat proliferative sickle cell retinopathy.
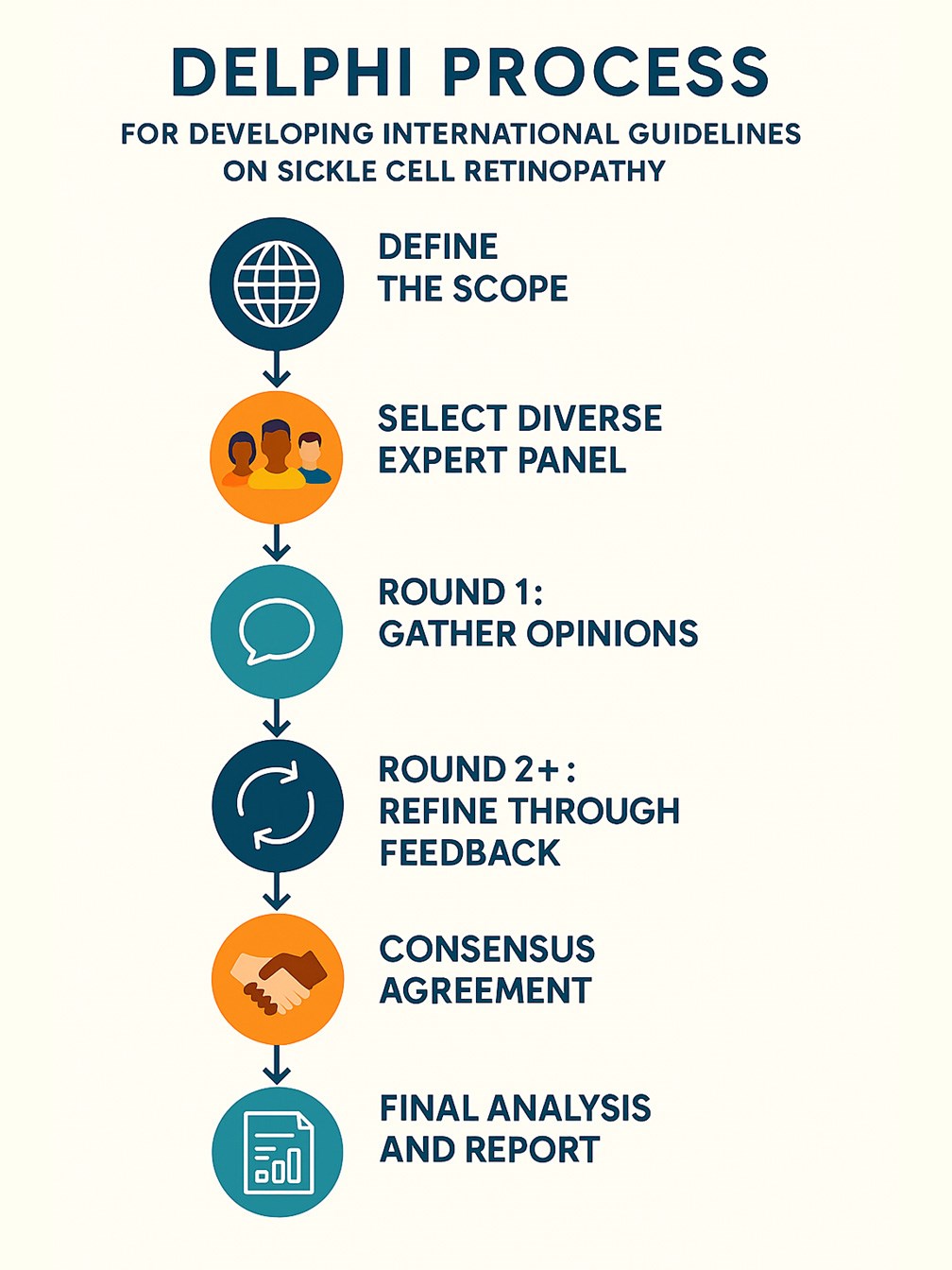
Figure 4: The Delphi process used by the SCR.net to develop international consensus guidelines for screening, diagnosis and management of SCR. The methodology includes scope definition, diverse expert recruitment, iterative rounds of feedback, and publication of agreed guidance.
The Delphi process involves structured, iterative rounds of questionnaires designed to capture expert consensus [9]. SCR.net has outlined the following steps (Figure 4):
- Define the scope: focused on developing international guidelines for SCR screening and treatment.
- Select a diverse expert panel: including ophthalmologists, haematologists, Delphi methodologists and participants from both high- and low-income countries.
- Round 1: capture opinions on current practice and unmet needs in SCR care.
- Round 2 and beyond: present anonymised group feedback, prompting panellists to revise their views until convergence is reached.
- Consensus definition: a predefined level of agreement (e.g. ≥70%) will determine inclusion in final guidance.
The Delphi is rooted in principles of epistemic justice by ensuring that those historically marginalised in global health research are not only participants but co-authors of the knowledge shaping care. By gathering and centring data from endemic regions, SCR.net challenges assumptions baked into existing paradigms, moving from a deficit-based model to one of global solidarity and shared value.
This work also centres the politics of knowledge production by challenging traditional power dynamics that have long dictated who gets to generate evidence and define ‘best practice’ [10]. SCR.net amplifies voices from the global south and it insists that those voices lead. By creating space for co-authorship of knowledge, this initiative rewrites who holds authority in retinal disease research.
For young people living with SCD, who are disproportionately impacted by SCR during their working years, vision loss represents a loss of opportunity, independence and dignity. Addressing SCR holistically as a public health, equity and socio-economic issue is core to SCR.net’s mission.
We are currently recruiting Delphi participants and through 2025 will launch our consensus study at key conferences across Africa and the Caribbean, including the African Retina Society (ARS) and the Ophthalmological Society of the West Indies (OSWI). We also intend to engage participants attending the Annual Scientific Conference on Sickle Cell and Thalassemia (ASCAT) conference in London.
We warmly welcome and invite clinicians, researchers and policy shapers from across the eye health and sickle cell communities. It would be great if we can collaboratively, respectfully and inclusively transform the narrative for SCR from neglect to equity, from silence to consensus and from marginalisation to co-leadership. That is the very essence of the work of the SCR.net. Please do join us.
For more information or to get involved, please visit: www.sicklecellretinopathy.net
References
1. Power-Hays A, McGann PT. When Actions Speak Louder Than Words — Racism and Sickle Cell Disease. N Engl J Med 2020;383(20):1902–3.
2. Smith WR, Valrie C, Sisler I. Structural Racism and Impact on Sickle Cell Disease: Sickle Cell Lives Matter. Hematol Oncol Clin North Am 2022;36(6):1063–76.
3. https://nhsrho.org/wp-content/uploads/2025/06/
SICKLE-CELL-COMPARATIVE-REPORT-.pdf
4. Thein SL, Howard J. How I treat the older adult with sickle cell disease. Blood 2018;132(17):1750–60.
https://www.sciencedirect.com/science/
article/pii/S000649712060653X
5. Amissah-Arthur KN, Mensah E. The past, present and future management of sickle cell retinopathy within an African context. Eye 2018;32(8):1304–14.
6. https://www.sicklecellretinopathy.net/
7. GBD 2021 Sickle Cell Disease Collaborators. Global, regional, and national prevalence and mortality burden of sickle cell disease, 2000-2021: a systematic analysis from the Global Burden of Disease Study 2021. Lancet Haematol 2023;10(8):e585-e599.
8. Fuseini MS, Gbedemah ZE, Ahmed A, et al. Global publication trends on sickle cell and diabetic retinopathy over eight decades: a highlight on information disparity: SCRnet consortium paper 1. Eye Open 1, 4 (2025).
9. Ramke J, Evans JR, Habtamu E, et al. Grand Challenges in global eye health: a global prioritisation process using Delphi method. Lancet Healthy Longev 2022;3(1):e31–e41.
10. Hardcastle F, Lyle K, Horton R, et al. The ethical challenges of diversifying genomic data: A qualitative evidence synthesis. Camb Prism Precis Med 2023;2:e1.
[All links last accessed May 2025]
Declaration of competing interests: None declared.






