A 21-year-old girl presented to her general practitioner (GP) with a three-month history of headaches, becoming more frequent and associated intermittent vomiting that did not improve with simple analgesics. There was a strong family history of migraines. She was initially diagnosed with migraine and given sumatriptan but returned within two weeks after no benefit.
On general examination, the patient appeared well with a grossly normal cranial nerve examination. However, confrontational field-testing by the GP did pick up bilateral inferior field defects and so the patient was advised to get an urgent ophthalmology review with formal visual field testing.
Ocular examination in eye casualty showed normal visual acuity and normal intraocular pressure bilaterally. There was no ophthalmoplegia; pupils were equally round and reactive to light without a relative afferent pupillary defect. Both fundi looked healthy with normal macula and vessels. Goldmann kinetic perimetry revealed a bitemporal hemianopia with more extensive field loss in the left eye.

Figure 1: Goldmann perimetry showing bitemporal visual field loss [4].
Because of the bitemporal visual field loss, there was a concern for compression of the optic chiasm and further closed questioning revealed fatigue, occasional dizziness and irregular periods all coming on around the same time as the headaches. Blood tests to assess thyroid and pituitary function were performed and the patient was referred to neuro-ophthalmology. Contrast-enhanced magnetic resonance imaging (MRI) of the patient’s brain was ordered.
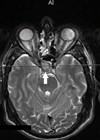
The MRI scan showed a large homogeneously enhancing suprasellar mass with bilateral extension, suggesting the possibility of a pituitary macroadenoma. Hormonal blood tests showed that it was a non-functioning pituitary adenoma with normal hormone levels. On the basis of all investigations, a clinical diagnosis of pituitary macroadenoma was made. The patient went on to have a successful surgical excision.
Discussion
This case highlights some key learning points. When the patient initially presented to her GP with chronic headaches associated with nausea and vomiting, migraine was a sensible top differential, especially given the family history.
Cranial nerve examination by the GP went on to reveal a bilateral inferior visual field defect. Visual field defects exist in 70% of patients with pituitary adenoma at the time of suspicion of the diagnosis due to pressure on the optic chiasm by the tumour [1]. Patients are usually unaware of this deficiency and this only becomes apparent during visual field testing [2]. Therefore, it is not uncommon for such a patient to be referred initially to ophthalmology by their GP.
Kinetic perimetry testing showed bitemporal field loss respecting the vertical meridian worse on the left side. Thus, the main concern was a suprasellar mass with compression of the optic chiasm. At this point, additional work-up such as blood tests to assess pituitary function, an MRI of the brain and referral to neuro-ophthalmology is indicated. Aside from a pituitary adenoma, other differentials for sellar masses to be aware of include craniopharyngioma and a parasellar meningioma.
Thinking about classification of pituitary tumours is helpful in directing these initial investigations and referral. Pituitary tumours are classified by size or by function [3]. Size is best determined by MRI and tumours >1cm in diameter are considered as macroadenomas. Function refers to whether there is any increase in pituitary hormone levels, with 50% of pituitary adenomas being prolactinomas (prolactin secreting tumours). Both of these are key determinants in deciding whether to trial medical therapy or go straight ahead to surgery.
References:
1. Dekkers OM, Pereira AM, Romijn JA. Treatment and follow-up of clinically nonfunctioning pituitary macroadenomas. J Clin Endocrinol Metab 2008;93(10):3717-26.
2. Jaffe CA. Clinically non-functioning pituitary adenoma. Pituitary 2006;9(4):317-21.
3. Davis JRE, Farrell WE, Clayton RN. Pituitary tumours. Reproduction 2001;121(3):363-71.
4. Rowe FJ, Rowlands A. Comparison of diagnostic accuracy between octopus 900 and goldmann kinetic visual fields. Biomed Res Int 2014;2014:214829.
COMMENTS ARE WELCOME

![Image showing Lateral view of the anatomy of the pituitary fossa, visual pathway and third ventricle [2].](/media/6855/eyejj17-cullen-figure-2.png?anchor=center&mode=crop&width=100&height=140&rnd=134172702910000000)

