History
-
A 31-year-old female patient presented with history of gradual downward displacement of the globe over the last six months.
-
The superotemporal mass then became palpable (Figure 1).
-
Lateral orbitotomy was performed following CT scans (Figure 2).
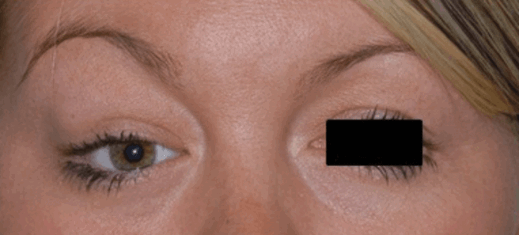
Figure 1.
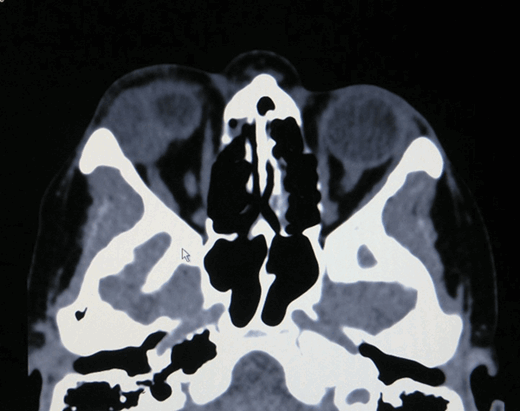
Figure 2.
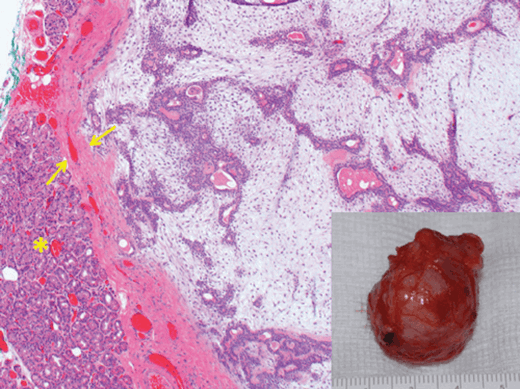
Figure 3.
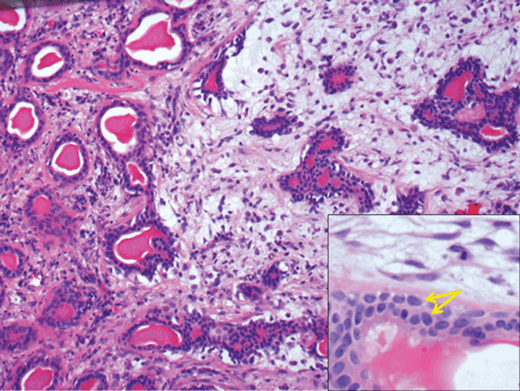
Figure 4.
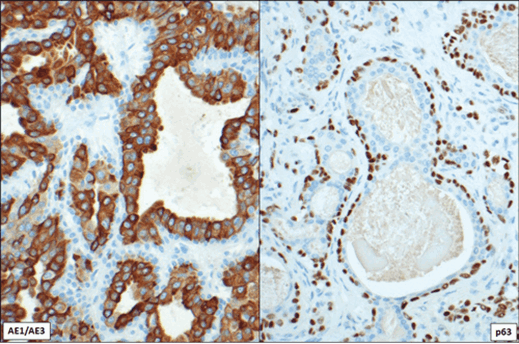
Figure 5.
Questions
-
How can Figure 2 be described?
-
Figure 3 shows the excised surgical specimen (inset) and a histological section of the lesion. What are the main features shown? What do the arrows and asterisk represent?
-
Describe Figure 4.
-
What are the markers highlighting on Figure 5? Which alternative markers could have been used instead?
-
Based on clinical features, histological and immunohistochemical findings, what is the most likely diagnosis?
Answers
1. CT scan showing well circumscribed heterogeneous mass in the right lacrimal gland area, displacing the globe.
2. The inset shows a well circumscribed nodular lesion. The histology section demonstrates a well circumscribed partly glandular partly myxoid lesion surrounded by a fibrous capsule (arrows). The asterisk shows adjacent normal lacrimal gland acini.
3. The image shows ducts and acini lined by epithelial and myoepithelial cells in a myxoid stroma to the right and a denser, collagenous stroma to the left. The arrows on the inset are pointing to dual cell layer in the acini. Inner epithelial cells and outer myoepithelial cells. Note the bland spindle stromal cells in the adjacent myxoid stroma.
4. AE1/AE3 (cytoplasmic and membranous staining) is highlighting inner epithelial cell layer and p63 (nuclear staining) is showing the outer myoepithelial cells. Alternative markers for epithelial cells: MNF116, CK7 or CAM5.2, and for myoepithelial cells: Alpha smooth muscle actin, S100, GFAP or caldesmon.
5. Pleomorphic adenoma.
COMMENTS ARE WELCOME


