History
-
A 48-year-old farmer with gradual worsening vision in her only eye was referred by her optician. She had recently moved to the UK and required an interpreter during consultation.
-
She seemed to have had vision problems since childhood. Although she was not certain of the diagnosis, she thought it was ‘contagious’ as other family members also had similar problems.
-
She had evisceration for endophthalmitis six months after a successful corneal graft in her country when she was 32. Although her vision improved after the corneal graft then, she did not want any further treatment to her only eye until she moved to the UK.
-
Examination confirmed widespread but well demarcated breadcrumb like confluent stromal deposits.
-
She went away to consider treatment options offered to her and on the following appointment she consented corneal transplantation to her only eye.
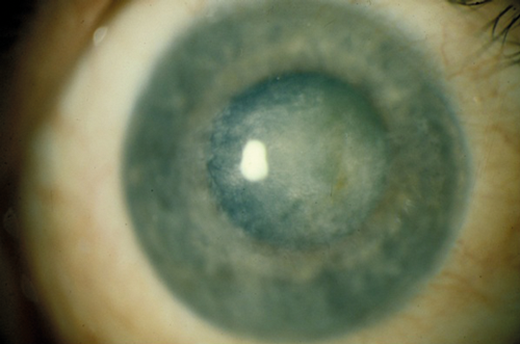
Figure 1.
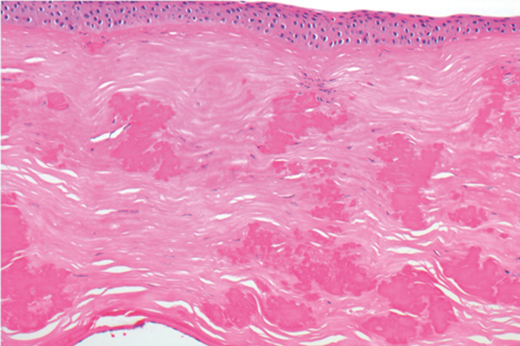
Figure 2.
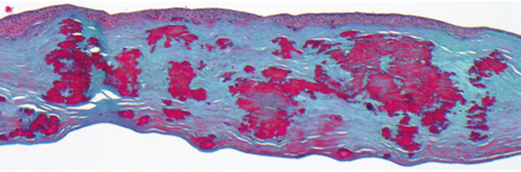
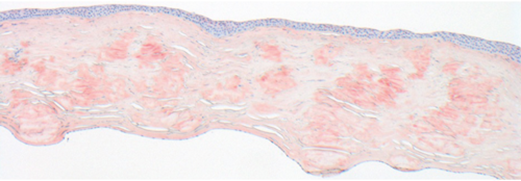
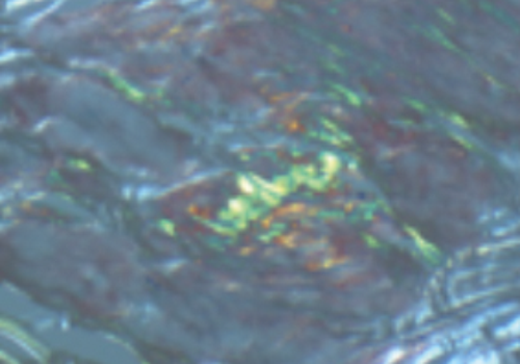
Figure 3. Top, Middle and bottom.
Questions
-
What does Figure 2 show?
-
Considering clinical information and features on Figures 1 and 2, what is the differential diagnosis?
-
Which special stain(s) would be helpful for confirming the diagnosis?
-
Figure 3 shows relevant special stains. What do they represent?
-
In this context what is the most likely diagnosis and what is the presumed genetic abnormality associated with it?
Answers
1. Penetrating keratoplasty specimen stained with hematoxylin & eosin and containing multiple eosinophilic deposits throughout the stroma. Bowman’s layer is lacking.
2. Epithelial-stromal corneal dystrophy including granular corneal dystrophy types 1 or 2. Based on Figure 2, lattice dystrophy also needs to be excluded.
3. Histopathological diagnosis requires Congo red and Masson trichrome stains at least.
4. Individual stromal deposits stain with Masson trichrome (top image) and / or Congo red (bottom image), suggesting presence of hyaline and amyloid deposits respectively. Congo red stained amyloid shows apple-green birefringence under polarised light (inset).
5. Granular corneal dystrophy type 2 (GCD2) or so called combined granular-lattice / Avellino dystrophy. GCD2 is associated with a mutation (most often R124H) in the transforming growth factor beta-induced (TGFBI) gene on 5q31.
COMMENTS ARE WELCOME


