History
An 18-month-old boy presented with a slow growing left anterior orbital lump medially. Examination revealed a palpable mass beneath the skin at the inferonasal aspect without any visual impairment. A CT scan (Figure 1) followed by an excisional biopsy was performed.
Questions
1. What does the arrow show (Figure 1)?
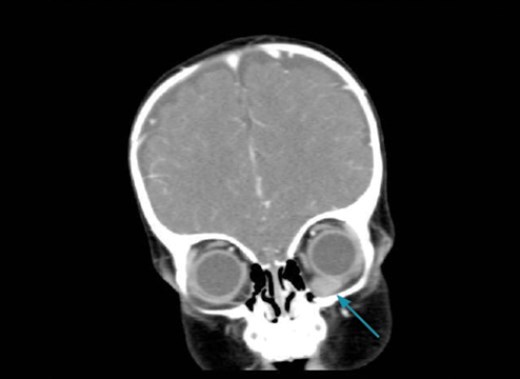
Figure 1.
2. What does Figure 2 (H&E) show and what are the arrows pointing to on Figure 3 (PAS)?
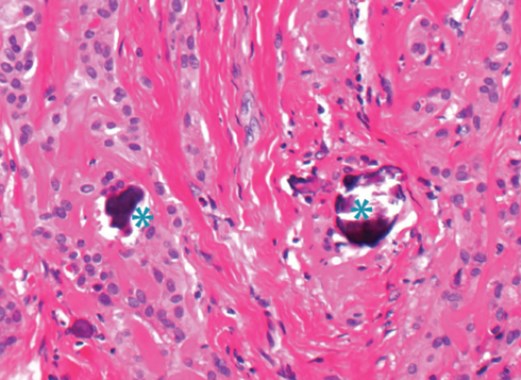
Figure 2.
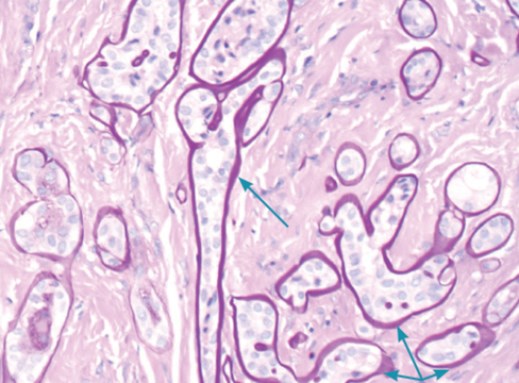
Figure 3.
3. Figure 4 shows immunohistochemistry for S100 and GFAP in which the brown staining represents positive expression by the epithelial cells. Which other markers may also be positive in this condition?
Figure 4.
4. Based on clinico-pathological features what is the diagnosis?
5. How is this lesion formed?
Answers
1. Coronal CT scan showing homogeneous mass in left inferonasal anterior orbital quadrant.
2. Figure 2 shows cords of epithelioid cells in a dense collagenous matrix. Focal dystrophic calcification is indicated by the blue marks. Figure 3 demonstrates thick basement membrane material produced by and enclosing the epithelial cells.
3. Epithelial cells of lenticular anlage express both S100 and GFAP but are also positive for vimentin and other antibodies against lens specific proteins (e.g. a-lens protein, b-crystallin). Conversely, lenticular epithelial cells do not express usual epithelial markers.
4. Phakomatous choristoma (also known as Zimmerman’s tumour).
5. Phakomatous choristoma is a congenital condition typically noticed in the first few months of life beneath the lower eyelid inferonasally. It consists of nests of lens epithelial-like cells present in an abnormal location (choristoma). The PAS-positive basement membrane material produced mimics lens capsule. The lesion probably originates from displacement of the lens placode into the deeper mesodermal tissue of the lower eyelid. The usual clinical differential diagnosis is a dermoid cyst.
COMMENTS ARE WELCOME


