History
A 40-year-old swimming instructor undergoes an enucleation for a blind painful eye. There is a history of soft contact lens wear. She has had a corneal abscess and corneal graft procedures in the past.
Questions
1. What does this immunohistochemical stain of cornea demonstrate (Figure 1)?
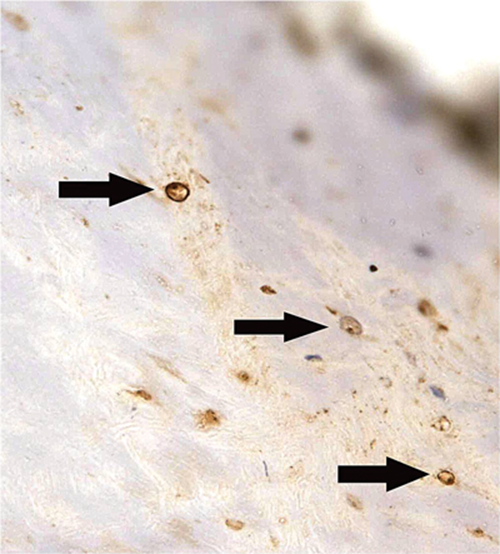
Figure 1.
2. What does this field including sclera and choroid show (Figure 2)?
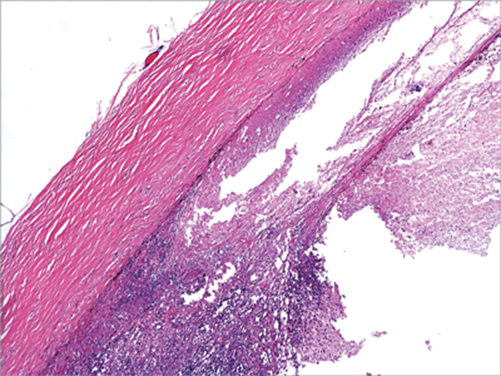
Figure 2.
3. What does this field including sclera and choroid show (Figure 3)?
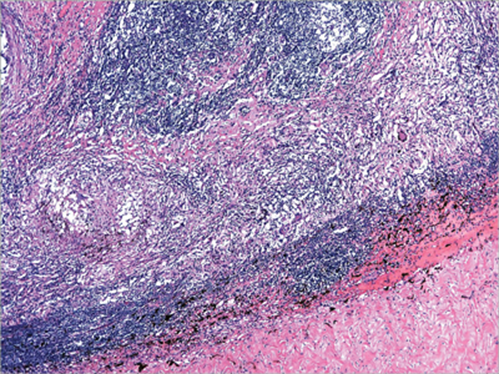
Figure 3.
4. What does this higher power field show (Figure 4)?
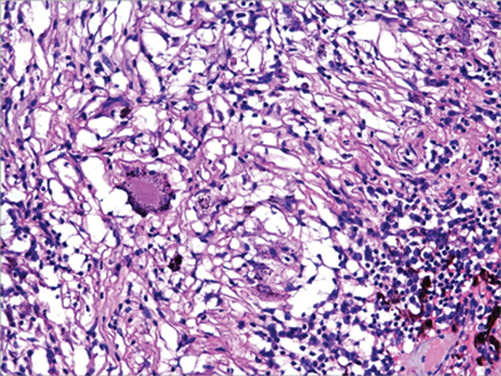
Figure 4.
5. What is the major clinical concern?
Answers
1. Acanthamoeba cysts.
2. Necrosis and inflammation consistent with acute endophthalmitis.
3. Granulomatous inflammation on a background of heavy lymphocytic infiltrate.
4. Multinucleate giant cells and pigment phagocytosis.
5. The granulomatous inflammation in the region of Bruch’s membrane raises the suspicion that this could be an exciting (inciting) eye in sympathetic ophthalmitis.
Discussion
This globe showed Acanthamoeba cysts within the cornea (but not the sclera or choroid), necrotising endophthalmitis with barely recognisable intraocular structures, and granulomatous inflammation which was located roughly in the region of the choroid. No other organisms were identified. The granulomata could conceivably have been part of the acute endophthalmitis process, but their location was highly suspicious of sympathetic ophthalmitis. Acanthamoeba infection may be associated with granulomatous inflammation, but endophthalmitis due to Acanthamoeba has only been reported a couple of times.
References
1. Castiblanco CP, Adelman RA. Sympathetic ophthalmia. Graefes Arch Clin Ex. Ophthalmol 2009;247:289-302.
2. Davis MJ, Packo KH, Epstein RJ, Grostern RJ, Cohen JA. Acanthamoeba endophthalmitis following penetrating keratoplasty for Acanthamoeba keratitis. Arch Ophthalmol 2010;128:505-6.
COMMENTS ARE WELCOME


