History
-
A 68-year-old female patient was referred from her GP with bilateral conjunctival lesions on her upper eyelids which cause local irritation and dry eyes.
-
Her past ophthalmic history is uneventful.
-
However, systemically she has history of high blood pressure and episodes of increasing shortness of breath.
-
On examination, she had several small pale lumps on upper eyelids (Figure 1).
-
A conjunctival biopsy was performed and material sent for ophthalmic pathology assessment.
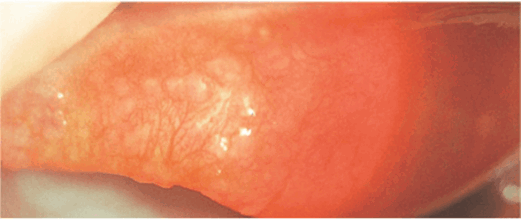
Figure 1.
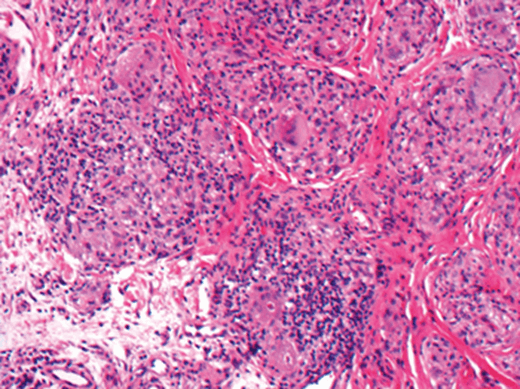
Figure 2a.
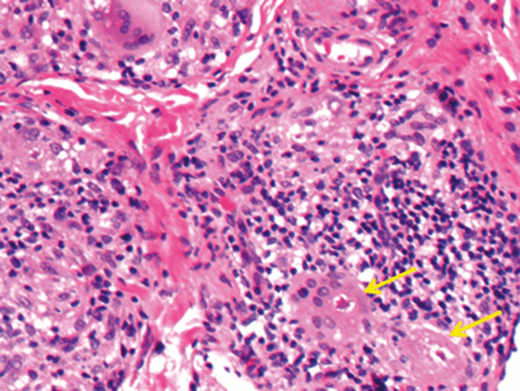
Figure 2b.
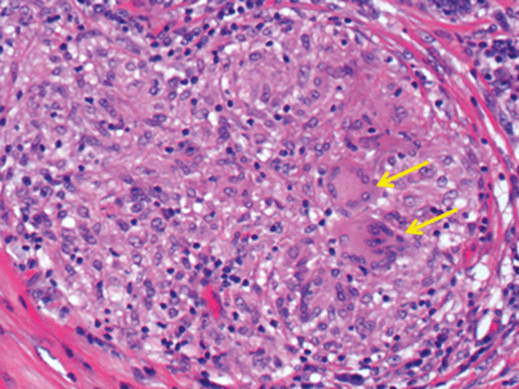
Figure 3.
Questions
-
Figure 2A shows a representative field of the biopsied material. What does it demonstrate?
-
What do the arrows show on Figures 2B and 3?
-
What is the morphological differential diagnosis? Are there any special stains which would help refining the diagnosis?
-
On follow-up the patient had chest x-ray done (due to her respiratory symptoms). The x-ray confirmed hilar adenopathy and reticulonodular infiltrate. She also had an abnormal blood test result. What was the likely test performed?
-
Taking together clinico-radiological features and morphological findings, what is the most likely diagnosis?
Answers
1. Well-defined non-necrotising epithelioid granulomas surrounded by mild fibrous bands and an inflammatory infiltrate.
2. Multinucleate giant cells. In Figure 2B the giant cells contain asteroid bodies (small, intracytoplasmic, eosinophilic star shaped structures) in their cytoplasm.
3. The main differential diagnoses are sarcoidosis, mycobacteriosis and fungal infection. Ziehl-Neelsen stain is required for the diagnosis of mycobacteriosis / tuberculosis and both periodic acid Schiff (PAS) and Grocott are helpful in confirming fungal infection.
4. Angiotensin converting enzyme (ACE). Serum ACE levels can be increased in this condition.
5. Sarcoidosis.
COMMENTS ARE WELCOME



