Cataract removal with intraocular lens (IOL) implantation is one of the most frequently performed surgeries in current clinical practice [1,2]. New microsurgical techniques and refined IOL power calculations allow excellent refractive outcomes.
Refractive surprise following cataract surgery is uncommon [1-3] and the literature on its causes is extensive. We describe a case of severe hypermetropic shift following cataract surgery caused by posterior capsular striae (PCS), a cause not mentioned in the literature.
Case report
A 72-year-old woman with a history of refractive eye surgery presented with blurred vision. Her refraction and visual acuity in the left eye were 0.75 (-0.75) 170° and 6/12 respectively. Slit-lamp examination revealed a nuclear cataract in that eye. The patient underwent phacoemulsification with implantation of a trifocal toric IOL in her left eye. IOL positioning was performed using Alcon’s© VERION™ Image Guided System. On day one postoperatively, she complained of blurred vision and the refraction in her left eye was +5.25 (-3.00) 20°. Slit-lamp examination revealed opacification and striae of the posterior capsule, but no corneal oedema or intraocular inflammation. The IOL was in the correct position and fundus examination was normal. Three days later, the refraction was unchanged, and PCS remained. Optical coherence tomography (OCT) revealed thickened, hyperreflective folds of the posterior capsule, in contact with the IOL (Figure 1).
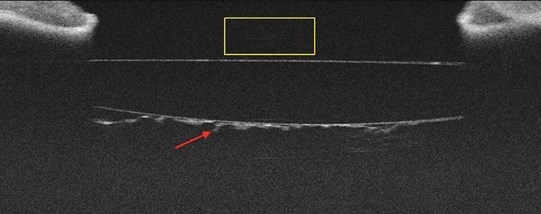
Figure 1: OCT image showing the posterior capsule wrinkled, thickened and added to the optics (red arrow).
Balanced salt solution was injected into the anterior chamber to expand it and flatten the striae. Although the patient reported a functional improvement within a few hours, the PCS had reappeared on OCT three days later, with additional central posterior capsule opacification (PCO). An urgent, central ND: YAG laser capsulotomy was performed in her left eye. The PCS disappeared immediately and permanently after the procedure, as shown on the OCT in Figure 2. The patient’s refraction returned to +0.5D with an uncorrected visual acuity of 6/6.
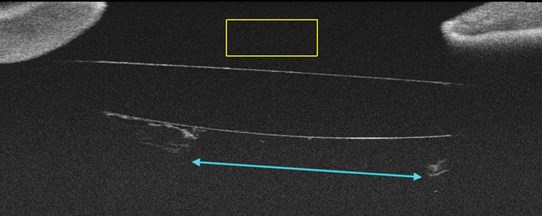
Figure 2: After capsulotomy, the central optic zone is released (blue arrow).
Comment
Although refractive surprise following cataract surgery is more uncommon with improving techniques and technologies, it remains a recognised complication of the operation. The Royal College of Ophthalmologists published an article on the causes of refractive surprise following cataract surgery and examples ranged from IOL subluxation to incorrect IOL power calculations [2]. The only cause specified as causing a hypermetropic shift was postoperative cystoid macular oedema and PCS were not mentioned. It is also widely recognised that previous corneal refractive surgery is a risk factor for poor refractive outcomes following cataract surgery [3]. Cochener and Arne state that, if postoperative hyperopia is superior to + 3D, one should suspect an IOL calculation error [3]. Once again, PCS are not mentioned.
There are few reports that discuss PCS in the literature. They are described as broad undulations that appear as single or multiple folds on the axis joining the apex of the genus of the haptics [4]. Some suggest that intraoperative PCS appear after implantation of an IOL into the capsular bag due to a size disparity between the IOL and bag [6]. The ability to measure the dimensions of the capsular bag preoperatively could offer the potential for more personalised IOL implantations. Most cases of PCS have been shown to disappear on their own and do not affect vision [5]. However, Wolken and Oetting suggest that the formation of linear PCO along persistent PCS in the visual axis may cause visual problems necessitating ND: YAG laser capsulotomy [6]. Nevertheless, the evidence of PCS leading to PCO and affecting vision is limited and contradictory. Our case demonstrates a rare cause of refractive surprise; clinicians should be aware that PCS can be a cause of refractive surprise, and that it can be managed with a central YAG laser capsulotomy.
References
1. Abdelghany AA, Alio JL. Surgical options for correction of refractive error following cataract surgery. Eye Vis (Lond) 2014;1:2.
2. Shalchi Z, Restori M, Flanagan D, Watson M. Managing refractive surprise. Focus 2018.
3. Cochener B, Arne JL: Refractive Surprise After Cataract Following Corneal Refractive Surgery. In: Alio J, Azar D (eds). Management of Complications in Refractive Surgery. Springer; 2018.
4. Vasavada AR, Trivedi RH. Posterior capsule striae. J Cataract Refract Surg 1999;25(11):1527‑31.
5. Awasthi N, Guo S, Wagner BJ. Posterior capsular opacification: A problem reduced but not yet eradicated. Arch Ophthalmol 2009;127(4):555-62.
6. Wolken MA, Oetting TA. Linear posterior capsule opacification with the AcrySof intraocular lens. J Cataract Refract Surg 2001;27(11):1889-91.
COMMENTS ARE WELCOME