Know’st thou the land where lemon-trees do bloom,
And oranges like gold in leafy gloom;
A gentle wind from deep blue heaven blows,
The myrtle thick, and high the laurel grows?
‘Tis there! ‘tis there,
O my beloved one, I with thee would go! [1]
When the Almighty created the Germans with all their many flaws and, to be fair, also a few virtues (both of which the British always seem to spot and appreciate best), he also made them homesick for Italy from the very start, as was never put into better words as the above by Goethe.
When I asked Mr Jon Park, former editor of this very column, whether he could provide me with an interesting case to present at one of the forthcoming vitreoretinal meetings, he kindly pointed me to the one I shall relate in a minute, on a gentleman on whom he had operated recently. His colleague from Nijmegen in the Netherlands, Niels Crama, with whom Jon had put me in touch, recommended the European VitreoRetinal Society Meeting (EVRS), as a great meeting to present this case as an edited video. Being the German I am, I could of course not resist this temptation, as the EVRS meeting took place in Italy that year, in beautiful Florence to be precise. And within Florence the organisers picked the most glamorous locations for dinners in pompous pallazzi and for the very interesting meeting itself, the Teatro della Pergola – truly one of the best meetings I ever attended.
a.
b.
c.
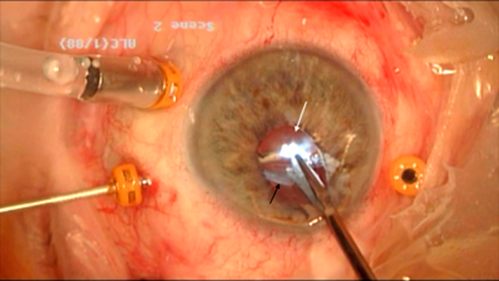
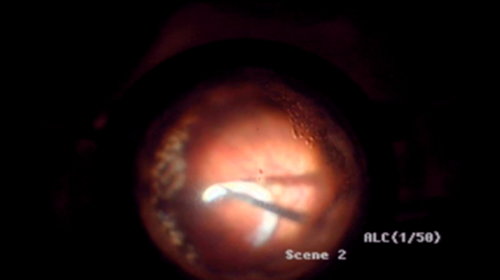
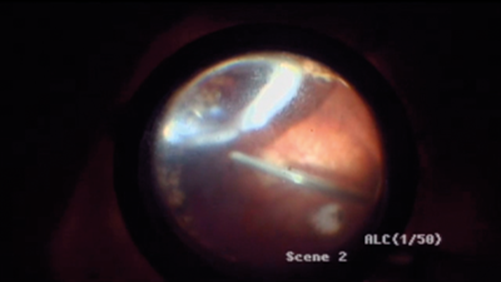
Figure 1: IOL (white arrow) removal with cutter and forceps trough a limbocorneal incision (a). Note the calcified Soemmerring’s ring that is separating at that moment (black arrow), falling back onto the retina (b), being eventually engaged with the fragmatome (c).
The case I presented told the story of a previously vitrectomised pseudophakic eye, in which the intraocular lens (IOL) was found to be dislocated into the vitreous cavity. The 23-year-old three-piece IOL was easy prey for removal with cutter and forceps through a limbo-corneal incision during a 23-gauge pars plana vitrectomy (Figure 1a). However, the remaining Soemmerring ring had calcified and decided not to come out with the IOL. Due to its irregular shape it could neither be removed easily with forceps (Figure 1b), nor destroyed by the cutter in the vitreous cavity. In the end, a 20-gauged fragmatome had to be used to fragment and remove the Soemmerring ring (Figure 1c).
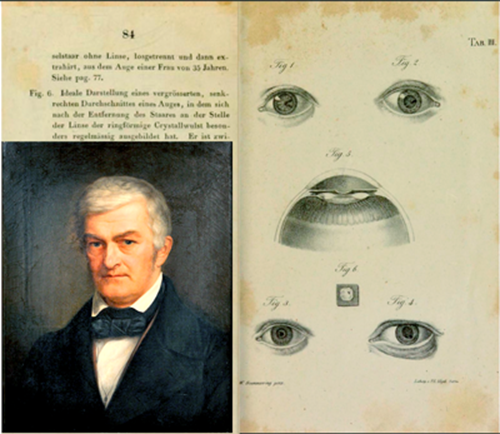
Figure 2: Detmar Wilhelm Soemmerring, 1793-1871, portrayed by Karl Friedrich von Strahlendorff
(bottom left) next to his first description of the ring that bears his name [2].
Soemmerring’s ring was named after Detmar Wilhelm Soemmerring, a German Ophthalmologist, who first described it in 1828 as a so called ‘Cristallwulst – crystal bead’ following traumatic or iatrogenic aphakia (Figure 2) [2]. Since Tooke’s article (which he actually published twice in different journals), we know more precisely that it is a proliferation of the remaining lenticular epithelial cells in the peripheral part of the capsular bag [3,4]. The fragmatome is typically used to emulsify crystalline lens material that dropped into the vitreous cavity just like a phaco probe does in the anterior segment (they both use ultrasound). But this case report shows how it can be used for calcified Soemmerring rings too that cannot be explanted by the conventional cutter or forceps approach. On a side note, it also tells a bit about the history of the German love affair for Italy.
References
1. Carlyle T. Wilhelm Meister’s apprenticeship and travels. Translated from the German of Goethe. London: Chapman and Hall; 1899:176.
2. Soemmerring W. Beobachtungen über die organischen Veränderungen im Auge nach Staaroperationen. Frankfurt am Main: Wilhelm Ludwig Wesché; 1828.
3. Tooke F. Dislocation of the Ring of Soemmering, its removal, with some notes on its pathology. Br J Ophthalmol 1933;17(8):466-76.
4. Tooke FT. Dislocation of the Ring of Soemmering, its removal, with some notes on Its pathology. Trans Am Ophthalmol Soc 1933;31:68-76.
Acknowledgments:
I am very grateful to the previous editor of this column, Mr Jon Park, now Consultant Ophthalmologist at Musgrove Park Hospital, Taunton, for providing this interesting case that I also presented at the 17th EVRS Meeting in 2017 in Florence, and to Mrs Silvia Bopp, Consultant Vitreoretinal Surgeon at MVZ Universitätsallee Bremen for helping with this report. We would all like to thank the patient for allowing the publication of his story.
COMMENTS ARE WELCOME





