History
-
A 57-year-old female patient presented with gradual painless diplopia over the last six months.
-
Examination revealed restricted upward eye movements and 4mm proptosis which did not increase with Valsalva manoeuvre.
-
Intraocular pressure was normal, no visual defects were noted, and fundus examination was unremarkable.
-
MRI scan (Figure 1) revealed a solid lesion occupying the extraconal space between medial rectus and superior rectus muscle.
-
Given the strong clinical suspicion of a neoplastic process, an excisional biopsy was performed and the specimen sent for ophthalmic histopathological assessment.
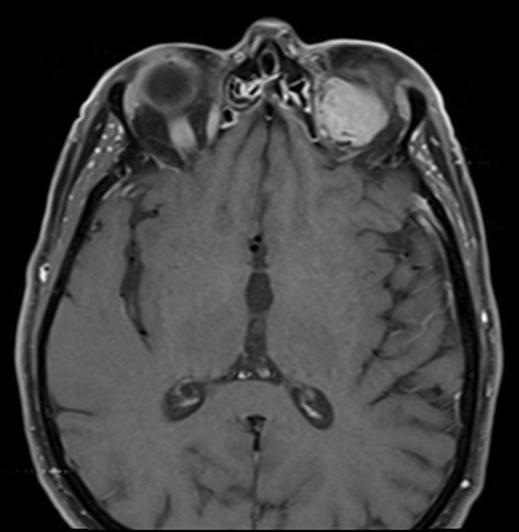
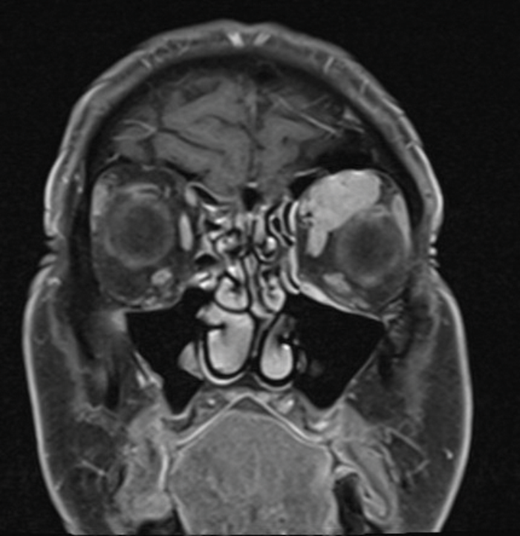
Figure 1 (top and above).
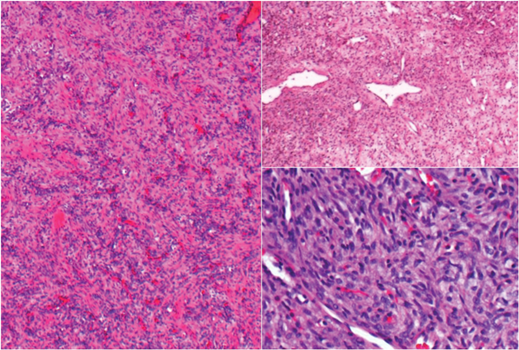 Figure 2.
Figure 2.
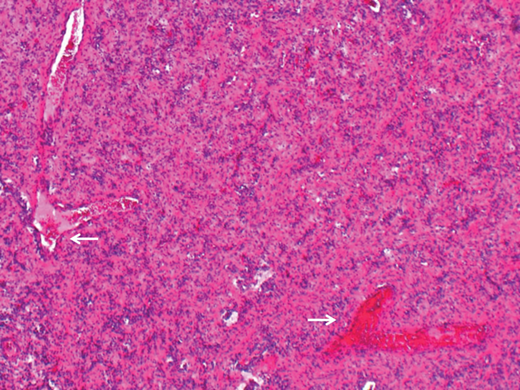
Figure 3.
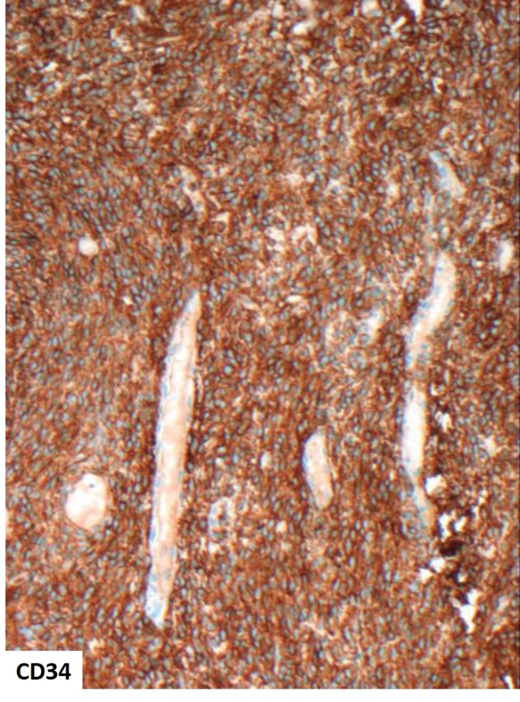
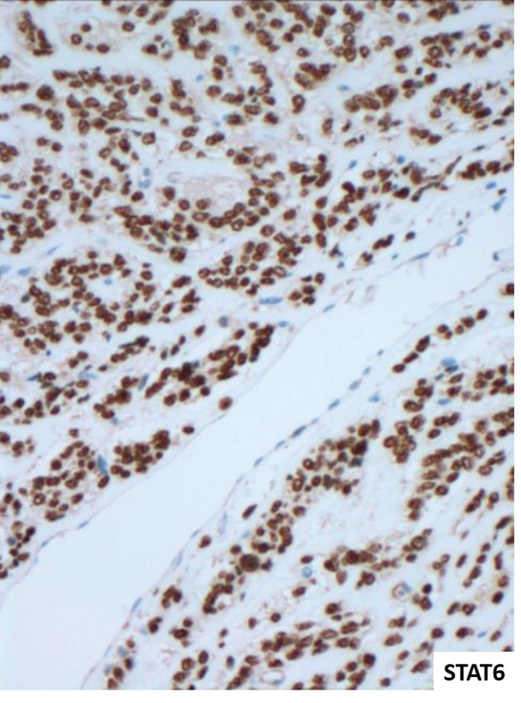
Figure 4 (top and above).
Questions
-
Considering clinical features and radiological presentation (Figure 1) what differential diagnoses would be considered?
-
What does the histology of the excised lesion (Figure 2) reveal?
-
What are the arrows pointing to (Figure 3)?
-
Immunohistochemistry on Figure 4 shows expression of CD34 (cytoplasmic) and STAT6 (nuclear). Are there any other markers also expected to be positive in this condition?
-
What is the most likely diagnosis?
-
What genetic abnormality would be expected to be present in this lesion?
-
Are there any morphological features associated with malignant behaviour?
Answers
1. The differential diagnosis of a solid orbital mass in an elderly patient includes lymphoproliferative disorders, vascular tumours, other primary soft tissue tumours and metastases. The lack of pain would make inflammatory / infective conditions less likely.
2. The H&E stained sections demonstrate a well vascularised and variably cellular spindle cell tumour. In areas the spindle cells are arranged in small fascicles.
3. Large branching (staghorn-like) blood vessels.
4. In addition to CD34 and STAT6 expression, BCL2, CD99 and GRIA2 are markers which may also be positive in this condition.
5. Solitary fibrous tumour (SFT).
6. NAB2-STAT6 gene fusion which results in overexpression of STAT6 (demonstrable on immunohistochemistry).
7. Diffuse hypercellularity, necrosis, cytological atypia and mitotic count over four per 10 high power fields may indicate malignant behaviour in SFT. Reassuringly none of these features were actually present in this case, although clinical surveillance would still be recommended.
COMMENTS ARE WELCOME
Would you like to comment on the topics raised within this article?
Email chris@pinpoint-scotland.com and, once approved, your comment will be published here.

