History
-
A 50-year-old female with a history of smoking, weight loss and cough presents to the ophthalmology clinic with a distorted pupil. Examination reveals a mass on the surface and within the iris (see Figure 1).
-
The ophthalmologists decide to biopsy the abnormal iris tissue, using a fine needle aspiration technique.
-
The biopsy is fixed in cytofixative and sent for an ophthalmic pathology opinion.
-
The stains used are mentioned with the figures.
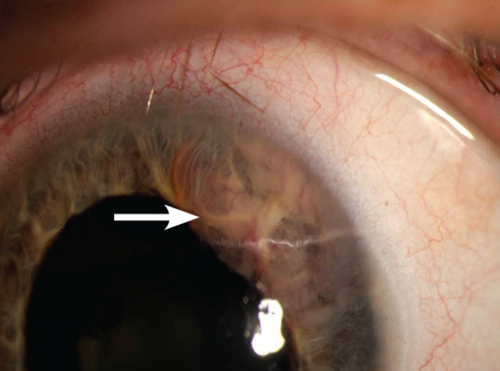
Figure 1.
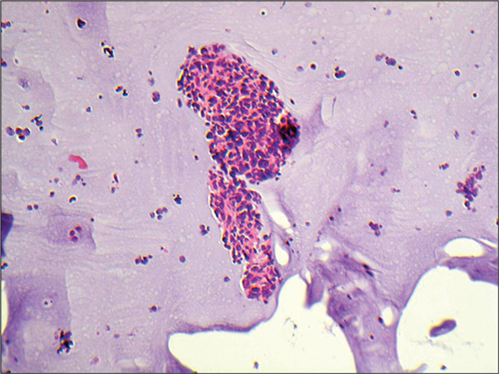
Figure 2: Haematoxylin and eosin stained biopsy.
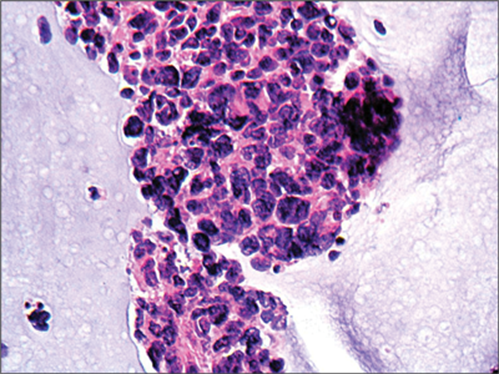
Figure 3: Haematoxylin and eosin stained sections of biopsy at higher power.
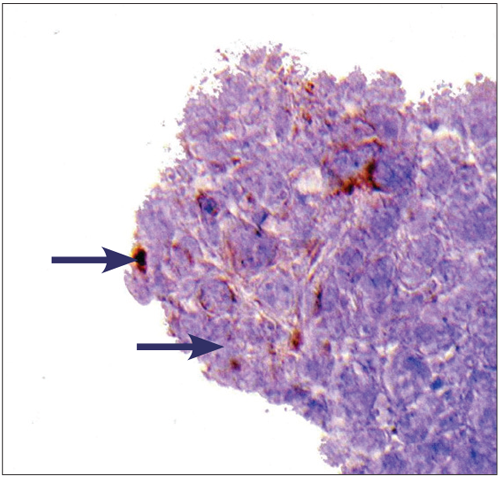
Figure 4: Cam5.2 immunohistochemistry showing some dot-like
paranuclear positivity (arrow) on some lesional cells.
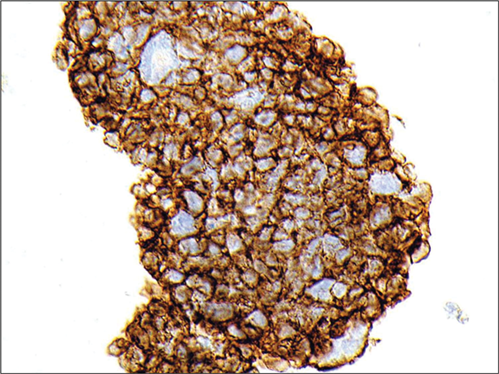
Figure 5: CD56 immunohistochemistry showing strong
circumferential staining with antibodies to N-CAM (CD56).
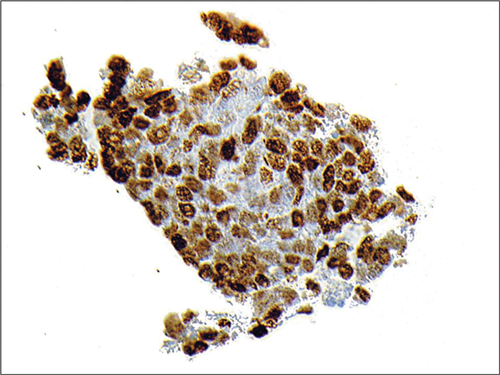
Figure 6: TTF-1 immunohistochemistry showing strong nuclear
staining with antibodies to thyroid transcription factor 1.
Questions
-
Given the history and the details of the lesion seen in the figures, is the diagnosis likely to be benign or malignant?
-
What do Figures 2 and 3 show?
-
What does Cam5.2 stain?
-
What is the significance of the staining seen in Figures 5 and 6?
-
What is the diagnosis?
-
What should happen next?
Answers
1. The history of cough, weight loss and smoking, coupled with a lesion in the iris, implies that the diagnosis is likely to be malignant.
2. Figures 2 and 3 show a small round blue cell malignancy, featuring cells in micro-biopsies and dispersed, with inconspicuous nucleoli, atypical nuclei with a salt and pepper ‘bitty’ chromatin pattern.
3. Cam5.2 stains low molecular weight cytokeratins 8 and 18 and is employed by histopathologists to stain a range of epithelial malignant neoplasms (carcinomas).
4. CD56 stains a cell surface protein called neural-cell adhesion molecule and positivity with this antibody implies neuroendocrine type differentiation. The presence of TTF-1 positivity indicates to the pathologist that the lesion has taken origin from the lung or thyroid.
5. The diagnosis is that of metastatic small cell carcinoma of the lung to the iris. Lung small cell carcinoma is a high grade, aggressive, neuroendocrine type carcinoma. This patient was diagnosed with lung small cell carcinoma previously and was treated with chemotherapy with good response.
6. This patient’s diagnosis requires review at a specialist ophthalmic pathology multidisciplinary meeting (MDT) and also at a specialist lung tumour MDT. The ophthalmic pathologist should ideally discuss his / her diagnosis with the lung pathologist who made the original diagnosis of lung small cell carcinoma for correlation purposes and audit. In this case, other metastases were identified subsequent to the iris biopsy.
COMMENTS ARE WELCOME



