
Current recommendations in the UK advise on wearing any facial covering to prevent the spread of the coronavirus [1]. Whilst this is vital for patient and hospital staff safety, it has led to several changes in the approach to a patient’s physical examination and management in clinical setting.
In several consultations at our ophthalmology department at the Northampton General Hospital (NGH), we have encountered cases of doubtful raised intraocular pressures (IOP) using the Goldmann applanation tonometry technique. A common factor noticed in these cases was the type of facial mask the patients presented with.
Case
Below we present a photograph taken whilst measuring the IOP of a patient who was wearing a respiratory protective FFP3 mask – a type of mask very commonly seen amongst out-patients.
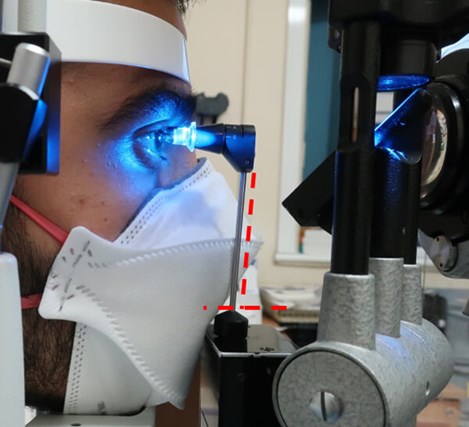
Figure 1: Photograph of a patient having his IOP checked with the Goldmann applanation tonometry technique. He is wearing a FFP3 mask. Note the tilt of the head of the tonometer. Due to a bulky mask this no longer is perpendicular to the eye as highlighted by the red dashed line.
Notice the tonometry head in relation to the mask – there is slight tilt of the head of the tonometer once it comes in contact with the mask. Consequently, in order to reach the cornea, the examiner will most likely apply more pressure and hence inadvertently, will obtain higher readings for the IOP.
Comment
Goldmann applanation tonometry is one of the most commonly used techniques for IOP measurement used in clinical setting.
A correct measurement requires a proper observer’s technique. One vital step is to ensure that the head of the tonometer is perpendicular to the eye. This is to guarantee that there is a full applanation of this device to the patient’s cornea and consequently an accurate result of the IOP [2].
Our observations have led us to believe that a bulkier mask can tilt the head of the device. This subsequently will lead to an overestimation of the IOP reading, which can have a significant impact on the patient’s management.
Without deemphasising the importance of the use of a facial mask, we believe it is imperative to take notice of the type of mask the patient wears and how this may affect the measurement of the IOP, as well as other ocular examination techniques.
We therefore advise our colleagues to reassess any cases of suspicious raised IOP that do not fit with the patient’s presentation and to consider if this could be explained by a more voluminous mask.
References
1. Public Health England. COVID-19:Guidance for the remobilisation of services within health and care settingsInfection prevention and control recommendations, 2020:
https://assets.publishing.service.gov.uk/
government/uploads/system/uploads/
attachment_data/file/910885/COVID-19
_Infection_prevention_and_control
_guidance_FINAL_PDF_20082020.pdf
(Last accessed December 2020).
2. Stevens S, Gilbert C, Astbury N. How to measure intraocular pressure: Applanation tonometry. Community Eye Heal J 2012;25(79-80):60.
COMMENTS ARE WELCOME



