Chalazia are chronic lipogranulomatous inflammations of the eyelid secondary to a blocked meibomian gland. Whilst most resolve spontaneously, certain chalazia warrant treatment. Options include incision and curettage (I&C), lesion excision, intralesional steroid injections, and botox injections [1].
I&C is usually the standard surgical treatment for persistent chalazia. However, there is a growing body of evidence for the use of intralesional TA as a less invasive alternative approach.
Case report
We report a case of a 35-year-old patient who was referred to the oculoplastics team for incision and curettage of a non-resolving chalazion despite conservative measures. Upon discussion with the consultant, a decision was made to trial treatment with intralesional triamcinolone acetonide (TA) injection in the first instance. The patient received an intralesional injection of 0.2mls of 40mg/ml TA. The injection was uncomplicated, and the patient was discharged with telephone follow-up in a month’s time.

Figure 1: Intralesional TA deposits on upper lid.
At the follow-up appointment, the patient reported two new white lesions in his right upper lid that appeared 10 days after the injection (Figure 1). No other symptoms were otherwise reported. It was explained that this most likely represented TA deposits and would likely spontaneously resolve, but the patient was keen for surgical excision of the lesions for cosmetic reasons.

Figure 2: Marking borders for excision.
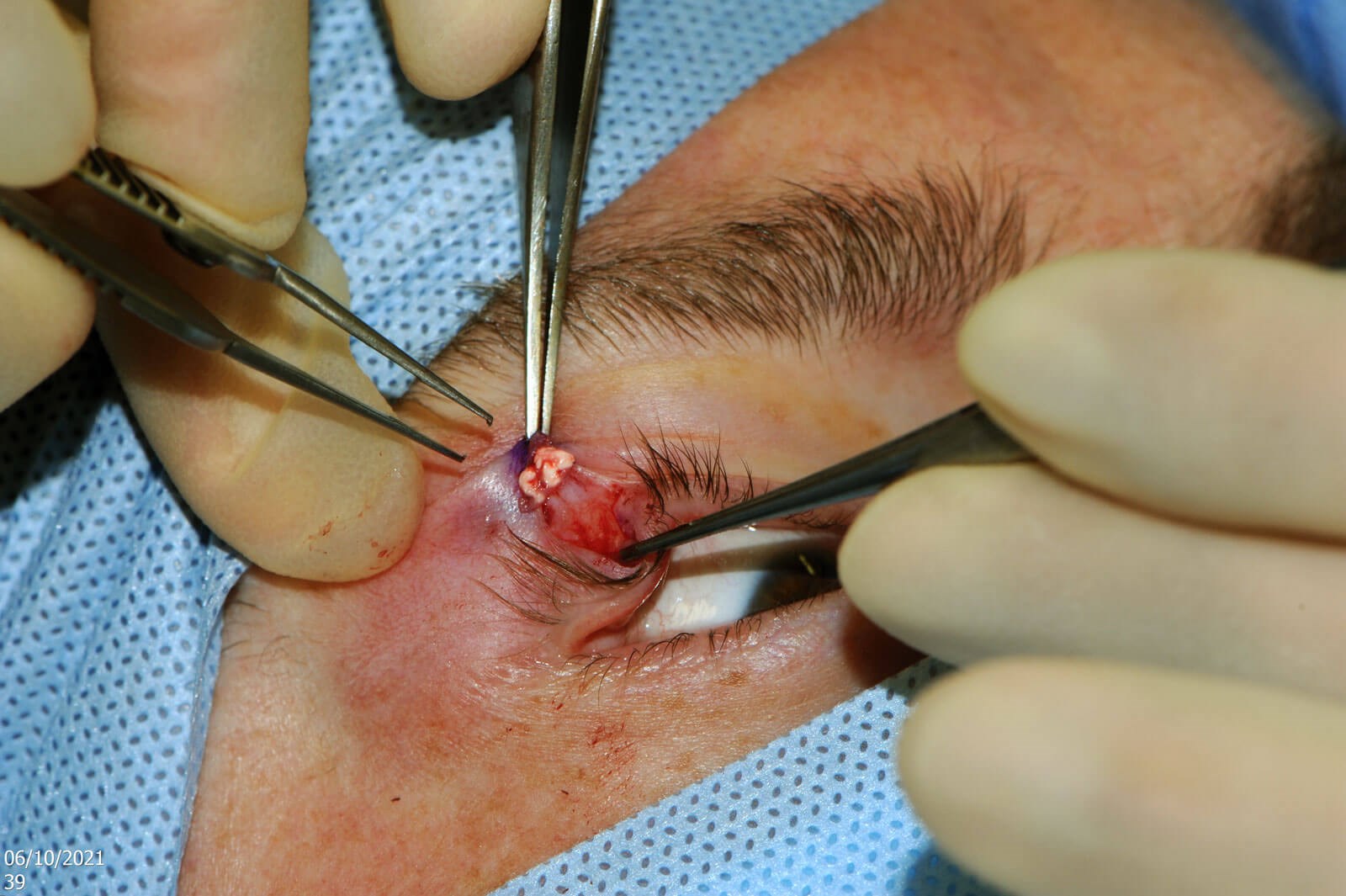
Figure 3: Exposed subcutaneous TA deposits.
The lesions were excised, and the samples sent for histology, which confirmed the presence of TA deposits (Figures 2 and 3).

Figure 4: Cosmetic result 10 days postoperatively.
The patient was reviewed 10 days later to ensure satisfactory outcome (Figure 4).
Comment
In a randomised controlled trial, Simon et al. found that intralesional triamcinolone acetonide (TA) injections were as effective as incision and curettage for primary chalazia [1]. This finding is echoed by similar randomised controlled trials by Goawalla et al., and Nabie et al. [2,3]. Goawall et al. went further by reporting a significant difference in patient acceptability between TA injections and I&C, with the former group being considered the least inconvenient [3].
TA deposition is well-described in the literature. In their study, Simon et al. enrolled 94 patients, 52 of whom received an intralesional injection of 0.1ml of 40mg/ml of TA. Six of those patients (11.5%) were found to have developed TA deposits following injection. In all six cases, the lesions spontaneously resolved within a few weeks [1]. Nabie et al. did a similar study comparing the effectiveness of intralesional TA injection with I&C. They also injected 0.1ml of 40mg/ml TA. However, they found TA deposition in 24 of 26 injected patients (92.3%) [2].
Nabie et al. commented on a further randomised controlled trial by Goawalla et al. In the latter study, they used an injection of 0.2ml of 10mg/ml of TA in 56 patients and reported no incidences of TA deposits. Nabie et al. suggested that this may be due to the lower concentration of TA used [2].
Another possible explanation for the TA deposits may be due to the clumping of TA crystals in the syringe. Therefore, one method of preventing TA deposits could be shaking of the syringe prior to injection.
Besides TA deposits, other important complications of intralesional TA injection include [1-3]:
- Local skin depigmentation and atrophy
- Retinal and choroidal vascular occlusion
- Inadvertently injecting into a sebaceous cell carcinoma
- Raised intraocular pressure.
Conclusion
Whilst I&C is appropriate in certain cases, the patient should be informed of the possibility of TA deposits if the immediate cosmetic result is likely to be a decisive factor, as there is faster resolution with I&C [2].
References
1. Simon GJB, Rosen N, Rosner M, Spierer A. Intralesional triamcinolone acetonide injection versus incision and curettage for primary chalazia: a prospective, randomized study. Am J Ophthalmol 2011;151(4):714-8.
2. Nabie R, Soleimani H, Nikniaz L, et al. A prospective randomized study comparing incision and curettage with injection of triamcinolone acetonide for chronic chalazia. J Curr Ophthalmol 2019;31(3):323-6.
3. Goawalla A, Lee V. A prospective randomized treatment study comparing three treatment options for chalazia: triamcinolone acetonide injections, incision and curettage and treatment with hot compresses. Clin Exp Ophthalmol 2007;35(8):706-12.
Declaration of competing interests: None declared.
COMMENTS ARE WELCOME





