Introduction
Sarcoidosis is a multisystem granulomatous inflammatory condition which predominantly affects the pulmonary system and intrathoracic lymph nodes, followed by ocular involvement [1].
We present an interesting patient who developed acute anterior uveitis and subsequent ciliary body granuloma clinically mimicking a melanoma as the primary manifestation of underlying systemic sarcoidosis.
Case report
Fit and well 28-year-old Caucasian man presented with a one-week history of painful, red, photophobic right eye. Systemic enquiry revealed fever, night sweats, cervical lymphadenopathy, reduced appetite, and unintentional weight loss for the past two weeks. He denied cough, dyspnoea, arthralgia and oral / genital ulcers.
Snellen visual acuity was right 6/7.5; left 6/5. Slit-lamp examination revealed circumlimbal injection with 2+ cells in the anterior chamber with otherwise clear media and normal fundus. Acute right anterior uveitis was diagnosed and he was treated with topical steroid and cycloplegic drops.
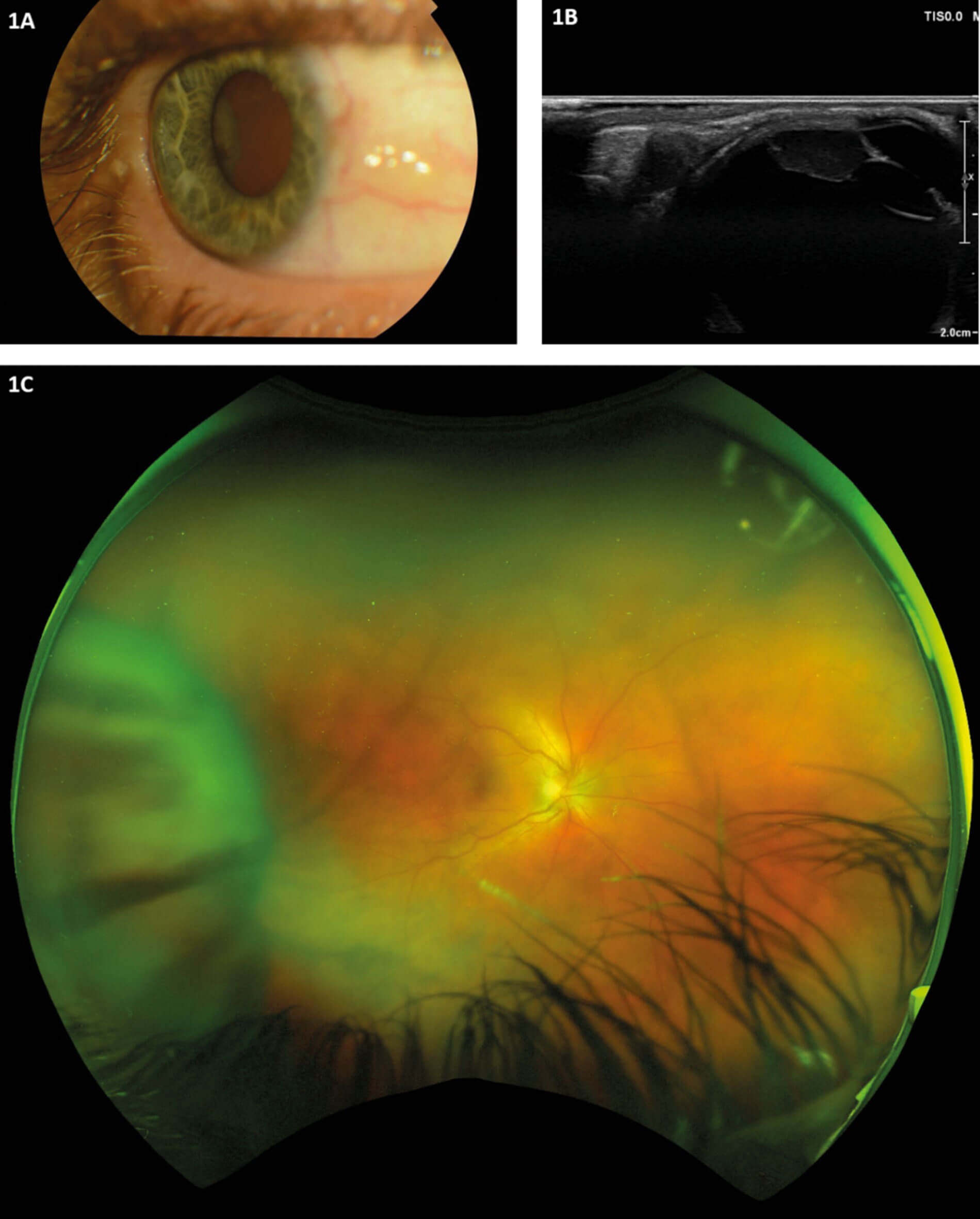
Figure 1A: Slit-lamp view of temporal ciliary body mass viewed through dilated pupil.
Figure 1B: UBM showing 9.9mm x 11.0mm x 4.5mm well-defined solid mass in the right eye continuous with the temporal ciliary body.
Figure 1C: Ultra-widefield fundus photo showing healthy retina with the temporal ciliary body mass visible anteriorly.
He returned to his scheduled clinic appointment four weeks later with persisting ocular and systemic symptoms. Examination revealed persistent right anterior uveitis with vitritis. A new ciliary body mass was seen temporally through dilated pupil (Figure 1A) and on fundus examination (Figure 1C). Relevant blood tests were obtained as shown in Table 1 and chest X-ray (Figure 2) was performed.
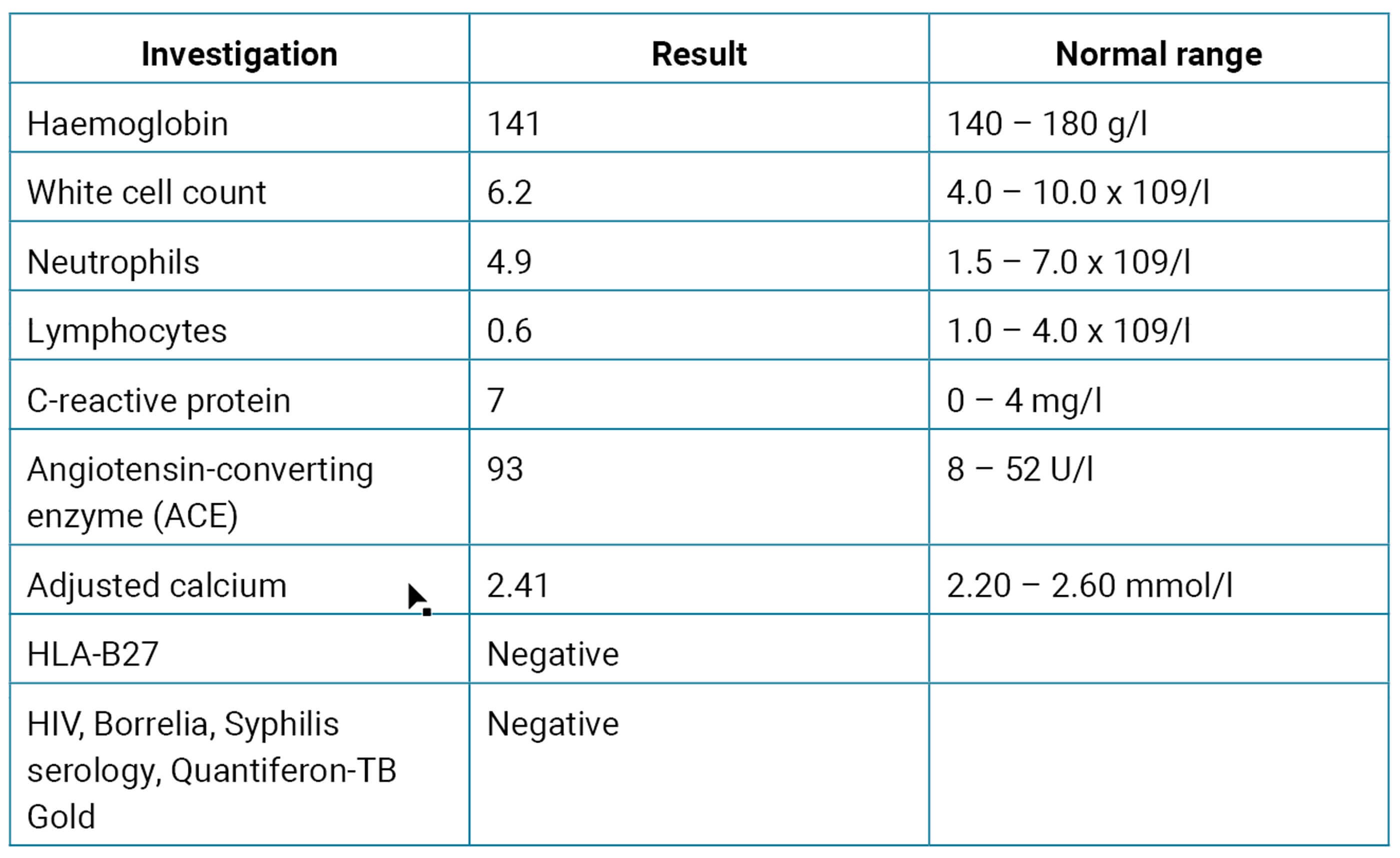
Table 1: Relevant blood results obtained to investigate for uveitis with systemic symptoms.
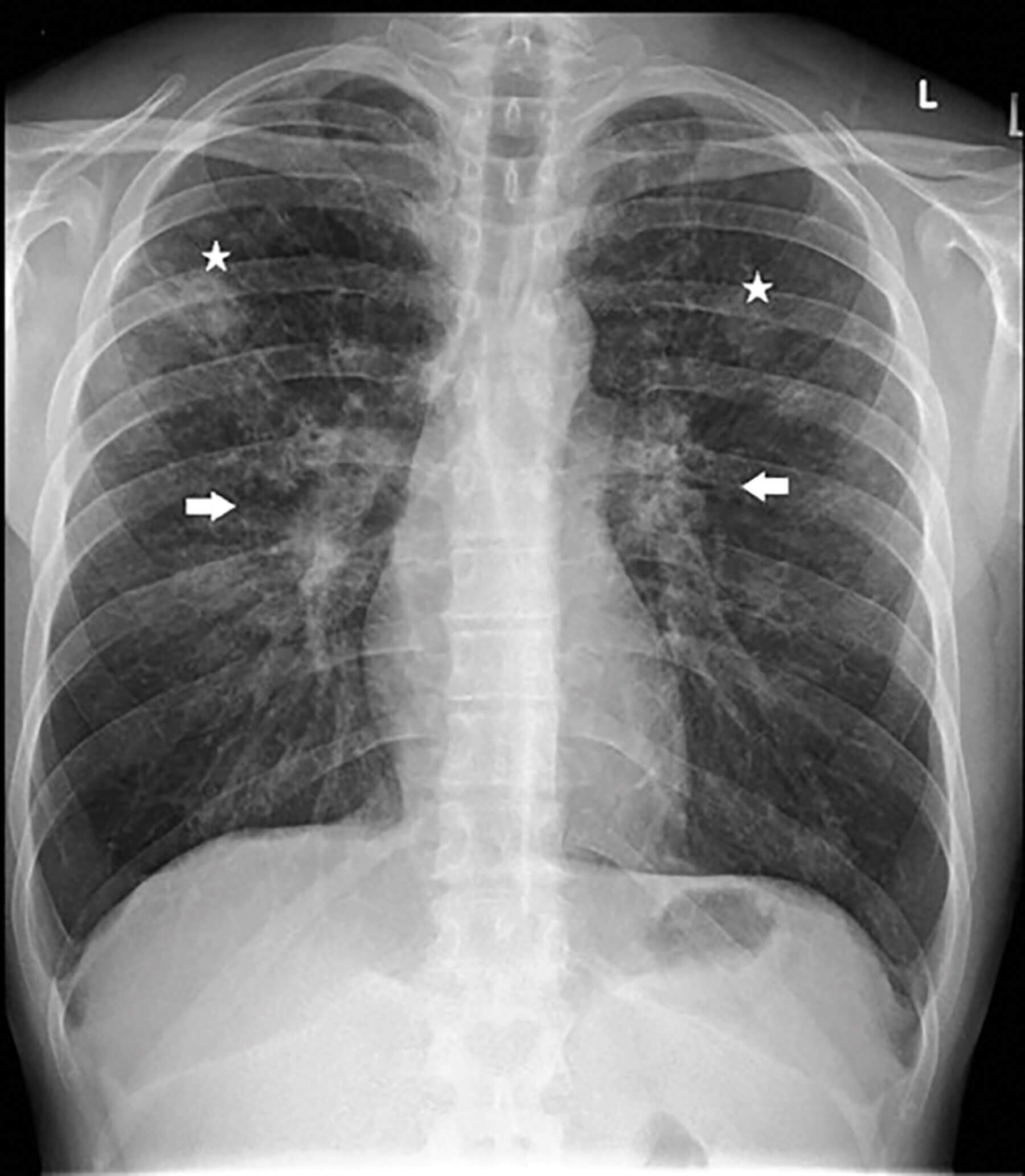
Figure 2: Chest X-ray showing nodular lung infiltrates (white asterisks) and bilateral hilar prominence
(white arrows). Note: Consent obtained from patient to publish case history and images.
Due to the suspicion of possible neoplasia, he was referred to the regional ocular oncology service for presumed melanoma. Ultrasound biomicroscopy (UBM) was performed and confirmed well-defined mass continuous with the ciliary body temporally (Figure 1B), suggestive of melanoma.
Subsequently, he also had chest high resolution computed tomography (HRCT) which revealed widespread nodular pulmonary lesions in the upper lung zones with extensive lymphadenopathy; indicative of pulmonary sarcoidosis.
Faced with diagnostic dilemma between inflammatory against neoplastic nature of the ciliary body mass, further discussion took place in a multidisciplinary team meeting. After re-reviewing the clinical findings, blood tests and chest imaging, the ciliary body mass was thought to be more likely an inflammatory granuloma secondary to systemic sarcoidosis instead of melanoma.
Patient received three days of 1g IV Methylprednisolone followed by oral steroids. His uveitis settled with significant reduction in the ciliary body mass size and complete resolution of his systemic symptoms. He was subsequently referred to respiratory team for further management of his systemic sarcoidosis.
Discussion
Uveal melanoma is the commonest primary intraocular malignancy in adults, with six percent being ciliary body subtype [2]. Ciliary body melanoma also has the worst prognosis being hidden behind iris, leading to delayed diagnosis combined with increased metastatic potential [3]. As such, ciliary body mass should always raise the suspicion of uveal melanoma and urgent referral to specialist centre is warranted.
UBM is an important ancillary test as it provides high resolution imaging of anterior segment, allowing visualisation of ciliary body pathology.
It is also vital to rule out other potential causes that could be contributing to our patient’s systemic symptoms. Normal white cell count and negative HIV serology made leukaemia and HIV unlikely. Negative Borrelia, syphilis serology and QuantiFERON suggested Lyme’s disease, syphilis, and tuberculosis are less likely. Serum ACE level whilst not diagnostic, is elevated in 60% of sarcoidosis patients [4].
Chest HRCT evaluates lesions seen on chest radiograph in greater detail and can detect parenchymal and mediastinal abnormalities. It revealed widespread pulmonary nodular lesions with extensive lymphadenopathy in our patient which are typical radiographic features of pulmonary sarcoidosis [5].
Whilst the authors agree that a positive tissue biopsy would be helpful to affirm our diagnosis, these investigations were thought to be more invasive and unlikely to affect patient’s management. As such, we have taken this pragmatic approach in the patient’s best interest.
In conclusion, ciliary body mass should always be investigated as potential uveal melanoma in the first instance. Clinicians should also be aware that uveitis can be a first manifestation of systemic sarcoidosis, with ciliary body granuloma being a potential rare finding in ocular sarcoidosis.
References
1. Ungprasert P, Ryu JH, Matteson EL. Clinical manifestations, diagnosis, and treatment of sarcoidosis. Mayo Clin Proc Innov Qual Outcomes 2019;3(3):358-75.
2. Xu TT, Moser JC, Dalvin LA. Uveal melanoma: laboratory advances and new frontiers in patient care. Curr Opin Ophthalmol 2021;32(3):301-8.
3. Costache M, Patrascu OM, Adrian D, et al. Ciliary body melanoma - a particularly rare type of ocular tumor. Case report and general considerations. Maedica (Buchar) 2013;8(4):360-4.
4. Bradley B, Branley HM, Egan JJ, et al. Interstitial lung disease guideline: the British Thoracic Society in collaboration with the Thoracic Society of Australia and New Zealand and the Irish Thoracic Society. Thorax 2008;63(Suppl 5):v1-58.
5. Criado E, Sánchez M, Ramírez J, et al. Pulmonary sarcoidosis: typical and atypical manifestations at high-resolution CT with pathologic correlation. Radiographics 2010;30(6):1567-86.
Declaration of competing interests: None declared.
COMMENTS ARE WELCOME




