Endogenous bacterial endophthalmitis (EBE) is a form of severe inflammation caused by haematogenous spread of a virulent bacterium from a nidus elsewhere in the body to intraocular tissues. It is a rare occurrence and only constitutes around 2–8% of all cases of endophthalmitis [1].
Panophthalmitis, frequently termed ‘endophthalmitis with orbital cellulitis’ is a further complication where there is purulent inflammation of all layers of the eye, including the Tenon’s capsule, and extending to the surrounding orbital structures. It is an ophthalmic emergency, and delayed treatment can have devastating consequences like severe permanent vision loss or evisceration of the eye.
Case report
A 73-year-old, bilaterally pseudophakic female with past ophthalmic history of bilateral age-related macular degeneration presented to the medical team at a district general hospital in May 2024. She had a 5–7-day history of red, severely painful left eye (LE) and visual loss down to light perception (LP) only.
Systemically, she also had symptoms of dysuria, increased urinary frequency and a new purulent cough for which she had been started on nitrofurantoin and amoxicillin respectively by her primary care provider. A urine culture sent five days prior to admission was positive for Escherichia Coli (E. coli) with over 100,000 organisms. Systemic workup proved negative for any further sources of infection apart from the urinary tract. Admission bloods showed raised inflammatory markers, with a white cell count of 18.43 × 10⁹/L and CRP of 227mg/L. Urine dip was positive for leucocytes and nitrites.

Figure: 1: Large left staghorn calculus demonstrated on a sagittal section of CT abdomen pelvis.
Her past medical history was significant for recurrent urinary tract infections (UTIs) and one previous hospital admission with urosepsis and E. coli bacteraemia. Imaging of the abdomen/pelvis had confirmed a long-standing left‐sided staghorn renal calculus (Figure 1), which she had previously declined to surgically treat.
On initial review in eye casualty, visual acuity was LP in the LE and 6/6-2 in the right eye (RE). Intraocular pressure was RE 10mmHg and LE 15mmHg. Relative afferent pupillary defect was negative for both eyes, but the left pupil was sluggish and small. Fibrin plaques were seen in the anterior chamber with no obvious hypopyon. B-scan showed no obvious vitreous opacification. Initial impression was anterior fibrinous uveitis. Treatment was commenced with intensive dilation, subconjunctival steroids, topical steroids and cycloplegics.
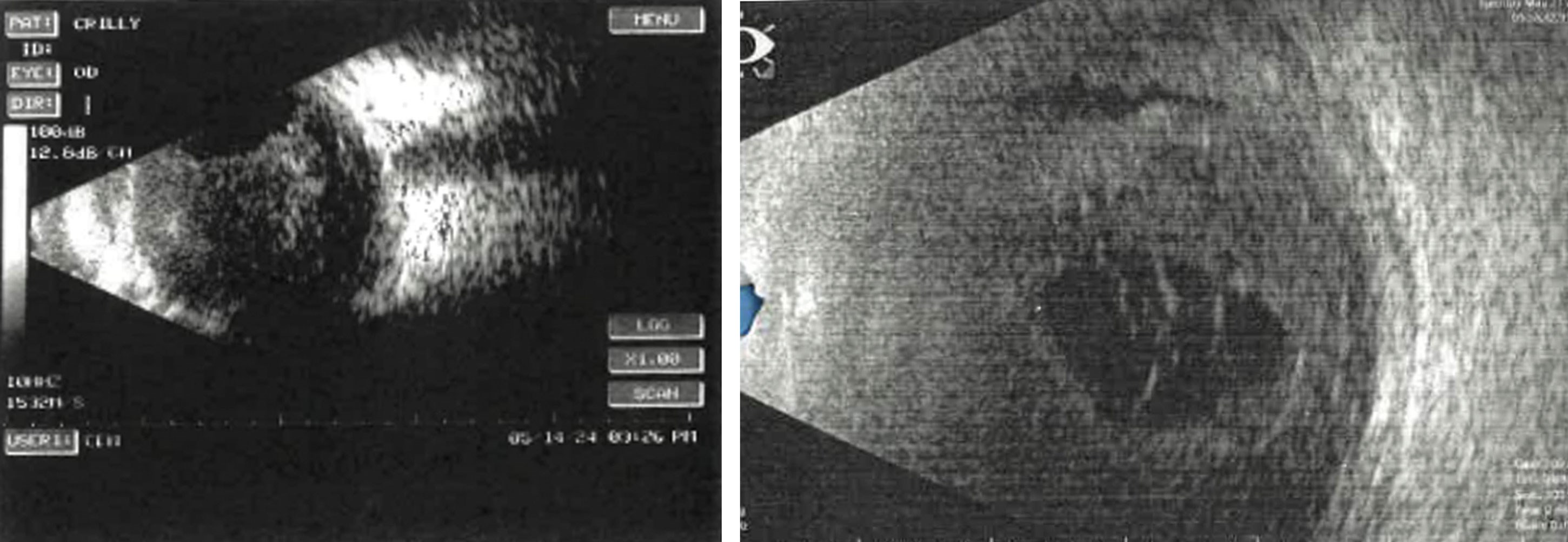
Figures 2 & 3: B scans taken during ophthalmology assessment. Left shows vitreous debris. Right shows loculated vitreous.
After 48 hours, fibrin plaques and pupil size improved. However, significant corneal oedema and several anterior chamber bullae were now present. Repeat B-scan demonstrated widespread vitreous condensation suggestive of vitritis (Figure 3). An anterior chamber and vitreous tap was undertaken. Intravitreal amikacin (0.1mL) and vancomycin (0.1mL) were administered. Topical moxifloxacin two-hourly from 06:00–22:00 was initiated alongside ongoing cyclopentolate and dexamethasone. The impression was changed to evolving endogenous endophthalmitis.
On subsequent ophthalmology review, anterior chamber inflammation persisted with fibrin and 2+ cells. Conjunctival chemosis was present 360°. No fundal view was available. B-scan demonstrated vitreous debris and loculated vitreous (Figures 2 & 3).
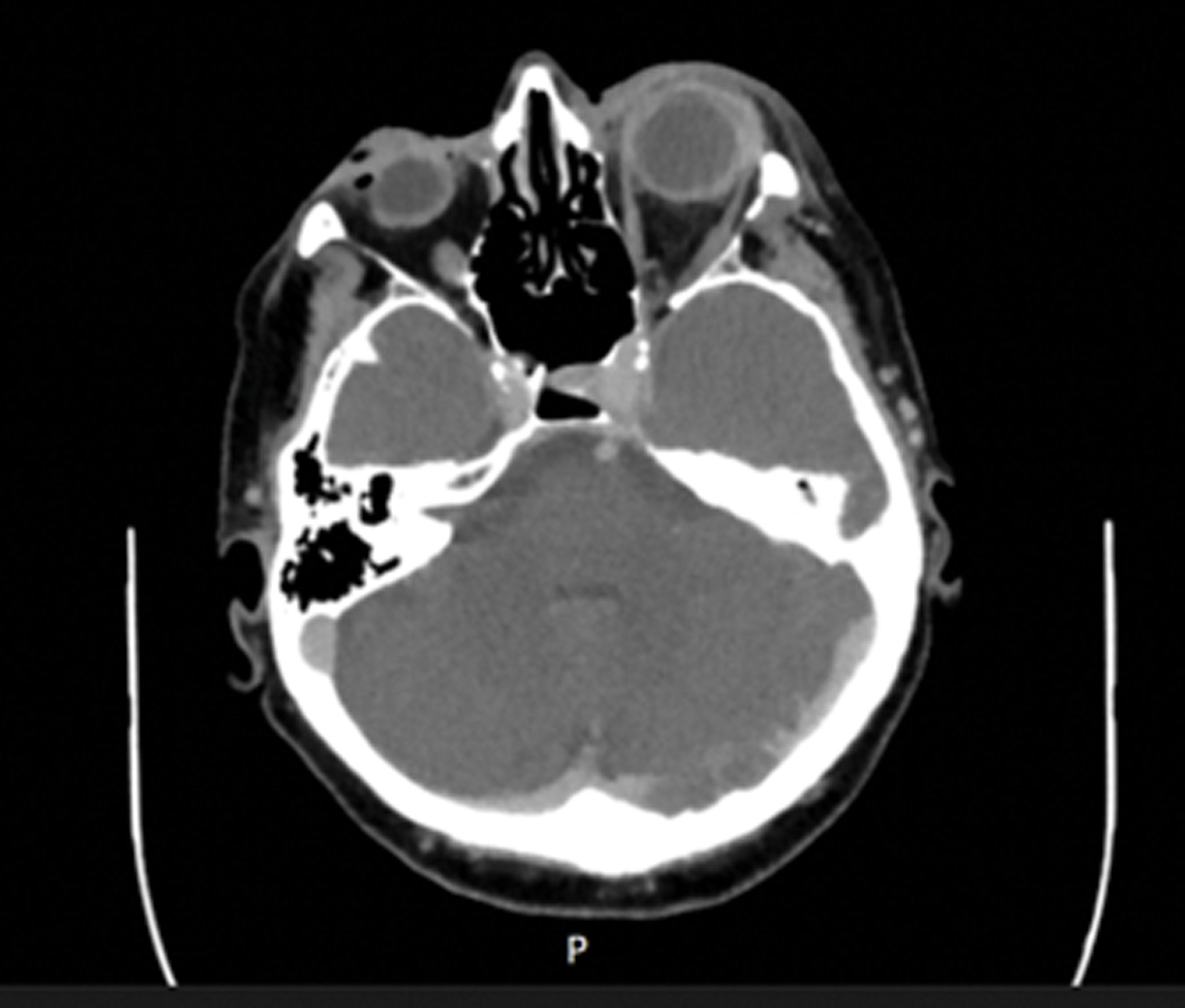
Figure 4: A sagittal section of the CT orbit.
Vitreous culture remained negative (later grew Brevibacterium casei, considered a contaminant). Moxifloxacin was reduced to six-hourly. CT of the orbit with thin cuts showed thickening of the sclera and choroid with reactive oedema along the orbital muscles (Figure 4). Given this, it was felt that the bacterial source had seeded into the choroid and loculated there – another reason for why the vitreous tap from earlier on had not grown anything.
During a subsequent review by ophthalmology, pressure in the LE was 42mmHg. She was started on PO Diamox and pressure-lowering drops with improvement in pressures to normal. An MRI orbit was ordered and reported diffuse thickening and enhancement of the entire left globe involving the sclera. Her antibiotics were changed from IV Co-Amoxiclav to IV Ceftriaxone for two weeks to cover an E. coli infection. After discussion with microbiology, oral moxifloxacin was added to the antibiotic regimen. Her inflammatory markers had improved to CRP 11 and WCC NAD on day 20 of admission.
Despite systemic improvement, vision in the left eye remained LP. The patient continued systemic/ocular therapy under close ophthalmology review. Urology follow-up was arranged to address the underlying staghorn calculus and recurrent UTIs.
Discussion
Endogenous panophthalmitis is exceptionally rare. Within the literature, the largest case series to date [2] analysed 342 published cases of endogenous bacterial endophthalmitis, highlighting several diagnostic challenges: delayed diagnosis occurred in up to 26% of patients, and nearly half presented without a view of the fundus. The urinary tract was identified as a major infectious source in ~6% of cases. Our case is consistent with these observations, with an initial impression of anterior uveitis prior to recognition of posterior segment involvement.
Anterior chamber and vitreous sampling are standard, though culture yield varies widely (40–60%) [2]. In our case, vitreous sampling was culture-negative, with Brevibacterium casei interpreted as a contaminant. Culture-negative endophthalmitis is well reported and may reflect prior antibiotic exposure [3]. Culture negativity does not exclude infection and should not delay treatment.
Management prioritises early intravitreal antibiotics, supported by systemic therapy. In this case, intravitreal amikacin and vancomycin were appropriately administered following suspicion of vitritis. Antibiotic escalation to systemic ceftriaxone was justified following CT-suggested panophthalmitis and urinary culture-confirmed E. coli. Although vitrectomy is often considered, its role in endogenous disease is debated [4]. Vitrectomy may reduce microbial load but is technically challenging when corneal oedema precludes posterior visualisation. In this case, anterior and posterior segment opacities limited meaningful surgical benefit.
Conclusion
Endogenous panophthalmitis is a rapidly progressive ocular emergency. This case demonstrates diagnostic difficulty and underscores the critical importance of comprehensive investigative workup. Identifying the systemic source is pivotal not only in managing ocular disease but potentially reducing the risk of life-threatening sepsis.
References
1. Okada AA, Johnson RP, Liles WC, et al. Endogenous bacterial endophthalmitis: report of a ten-year retrospective study. Ophthalmology 1994;101(5):832–8.
2. Jackson TL, Paraskevopoulos T, Georgalas I. Systematic review of 342 cases of endogenous bacterial endophthalmitis. Surv Ophthalmol 2014;59(6):627–35.
3. Durand ML. Bacterial and fungal endophthalmitis. Clin Microbiol Rev 2017;30(3):597–613.
4. Relhan N, Forster RK, Flynn HW Jr. Endophthalmitis: then and now. Am J Ophthalmol 2018;187:20–7.
Declaration of competing interests: None declared.




