COVID-19 is being investigated as a potential cause for various ocular diseases, with growing evidence of related retinal vascular changes, that vary from isolated cotton wool spots and retinal haemorrhages to retinal vascular occlusions [1.2]. COVID-related macular affection has also been reported where there are some recent case reports of acute macular neuroretinopathy (AMN) and paracentral acute middle maculopathy (PAMM) [3,4,5].
We report a case of a young patient with bilateral AMN-like maculopathy following recent diagnosis of COVID-19 infection.
Case
A 19-year-old patient presented to our emergency eye clinic with acute blurring of vision in both eyes, more in the left eye, for a few days. She had tested positive for COVID-19 by PCR 11 days ago. Past history was unremarkable apart from oral contraceptive pills intake for around two years. Her best corrected visual acuity was 0.08 in the right eye and 0.38 in the left eye ‘log Mar’.
Anterior segment examination was unremarkable, whereas fundus examination revealed macular changes in both eyes, more in the left eye, in the form of irregular reddish brown / grayish areas. There was no abnormality involving the rest of the retina (Figure 1).

Figure 1: Widefield multicolour photo of right eye and left eye showing irregular reddish brown
/ grayish area involving the macula of both eyes more extensive in the left eye.
The affected macular areas appeared hyporeflective on near infrared reflectance (NIR) images and spectral domain optical coherence tomography (SD-OCT) scans showed thickening of the outer plexiform layer with corresponding disruption of the ellipsoid zone. The changes were more extensive in the left eye, whereas in the right eye most of the temporal macular area was spared. The choroidal thickness was also noticed to be increased (Figure 2).
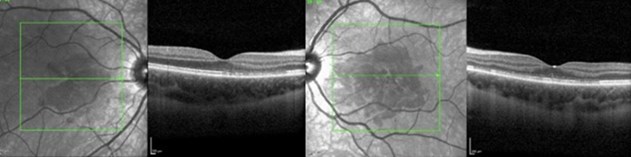
Figure 2: Near infrared reflectance revealed irregular area of decreased reflectivity more extensive in the left eye and
corresponding well to the areas of OPL thickening and EZ disruption on SD- OCT. The choroidal thickness was also increased.
Discussion
There is growing knowledge of SARS-CoV-2 ocular manifestations ranging from conjunctivitis to posterior ischaemic optic neuropathy [1,2]. Recent studies have reported a few cases of bilateral macular affection associated with COVID-19 infection and vaccination including PAMM and AMN [3,4,5].
AMN is a rare retinal disorder with a possible microvascular pathology affecting the deep capillary plexus. It mostly affects young females. Predisposing factors include viral illness or fever (48%), and oral contraceptive use (36%). The classic findings are reddish-brown petaloid lesions surrounding the fovea with hyporeflectivity on near infrared (NIR) imaging and are bilateral in approximately half of patients. Corresponding abnormalities of the outer plexiform layer (OPL), outer nuclear layer (ONL) and ellipsoid zone (EZ) are often present on SD-OCT [3,4,5]. There is no clear treatment for AMN and limited data on outcomes of AMN secondary to COVID-19. Despite sharing some of the characteristics of AMN, the case we report above shows more extensive macular changes than the previously reported COVID-related AMN cases and lacks the classic petaloid appearance. The patient’s presenting complaint was blurry vision rather than the typical scotoma.
COVID-19 is most likely the cause for her maculopathy, given that her symptoms started days after having positive PCR results for symptomatic COVID-19. The combination of possible hypercoagulability secondary to oral contraceptives as well as COVID-19 infection may have resulted in this extent of bilateral lesions in our patient. It is important to study whether short-term discontinuation of oral contraceptives should be considered to prevent further ischaemic compromise.
As our patient was unvaccinated against COVID-19, it may also be important to assess whether vaccination status has an effect on the extent of macular involvement. The case highlights SARS-CoV-2 infection as a possible cause for bilateral maculopathy. However, more studies involving larger numbers of cases are needed for better understanding of the association and the prognosis, particularly with the emergence of new variants.
References:
1. Nasiri N, Sharifi H, Bazrafshan A, et al. Ocular manifestations of Covid-19: a systematic review and meta-analysis. J Ophthalmic Vis Res 2021;16:103-12.
2. Sheth J, Narayanan R, Goyal J, Goyal V. Retinal vein occlusion in COVID-19: a novel entity. Indian J Ophthalmol 2020;68(10):2291-3.
3. David JA, Fivgas GD. Acute macular neuroretinopathy associated with COVID-19 infection. Am J Ophthalmol Case Rep 2021;24:101232.
4. Virgo J, Mohamed M. Paracentral acute middle maculopathy and acute macular neuroretinopathy following SARS-CoV-2 infection. Eye 2020;34:2352-3.
5. Drüke D, Pleyer U, Hoerauf H, et al. Acute macular neuroretinopathy (AMN) following COVID-19 vaccination. Am J Ophthalmol Case Rep 2021;24:101207.
Declaration of competing interests: None declared.
COMMENTS ARE WELCOME



