Patients who underwent vision correction in their 20s to 40s are now entering their 50s and 60s, the typical starting age for cataract development [1]. Consequently, ophthalmologists are increasingly encountering patients whose corneal profiles have been surgically altered, requiring advanced intraocular lens (IOL) assessment and customised surgical planning [2].
This patient population presents unique challenges: the disrupted anterior-posterior corneal power ratio invalidates standard keratometry assumptions [3,4], and traditional IOL formulae can produce refractive errors >1 diopter (D) in 30–40% of cases [3,5]. Moreover, post-refractive patients often have high visual expectations and are less tolerant of refractive surprise; failure to achieve spectacle independence can drive dissatisfaction even with good acuity [1].
Understanding previous refractive procedures
The key to successful IOL selection is understanding how each refractive surgery type alters corneal anatomy. Laser-assisted in situ keratomileusis (LASIK), photorefractive keratectomy (PRK) and keratorefractive lenticule extraction differ in surgical approach but have similar optical consequences. They alter anterior corneal curvature (ablation with or without a flap or lenticule removal), producing central corneal flattening for myopic treatments and central steepening for hyperopic corrections. These changes disrupt the anterior–posterior corneal ratio and asphericity, undermining standard keratometry and increasing the risk of refractive surprise if not accounted for.
Radial keratotomy (RK), widely performed in the 1980s, used deep radial incisions to induce central corneal flattening. Key issues include diurnal fluctuation (up to 1–2D in up to 60% of patients) and long-term hyperopic drift (reported in up to 43% of cases) [6,7].
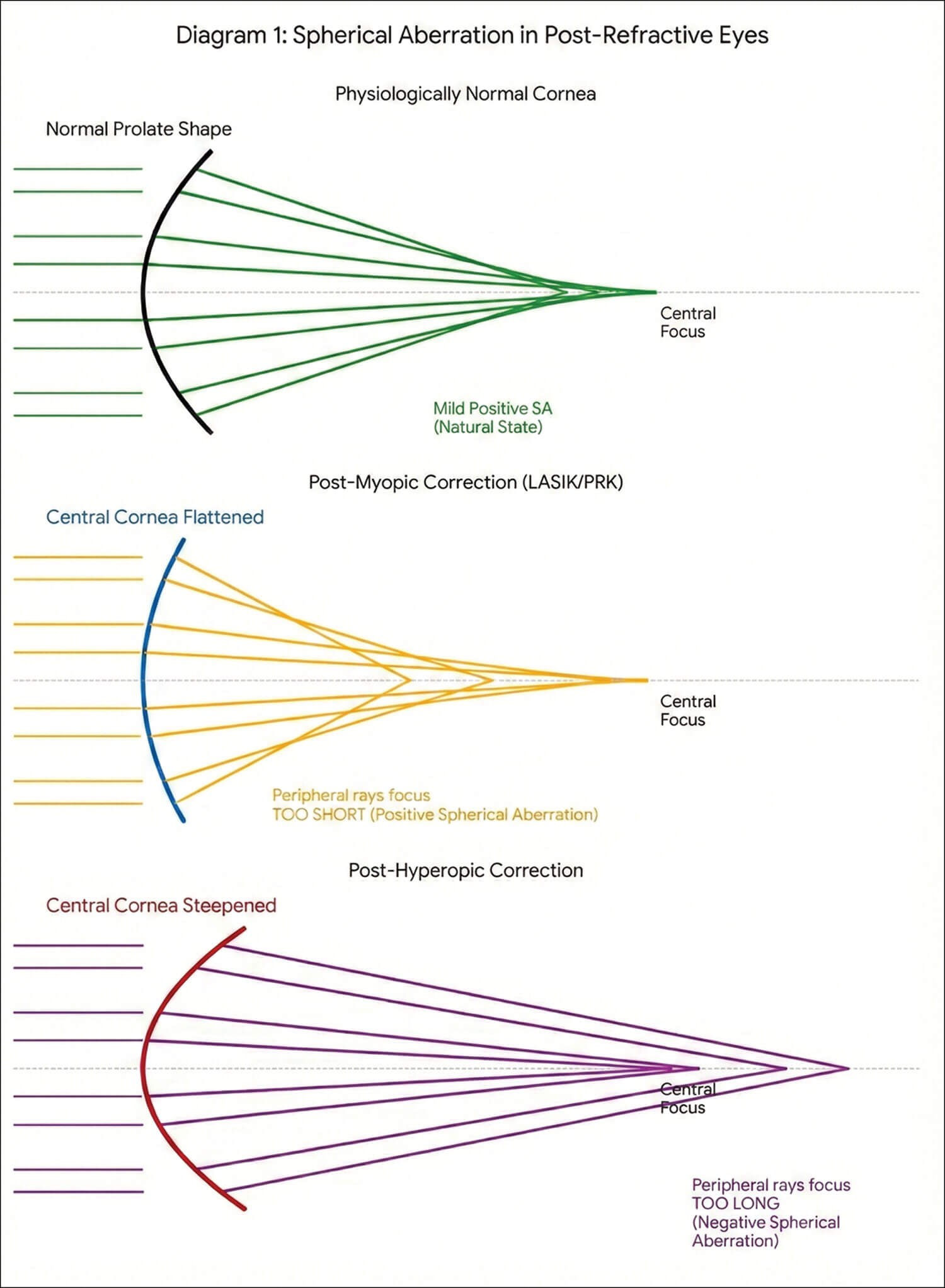
Figure 1: Spherical aberration in post-refractive eyes
(image generated using Gemini 3 Flash Image AI, Google, 2026).
Optical background and aberrations
The cornea contributes around 2/3 of the total refractive power of the eye [8]. Post-refractive surgery alters corneal asphericity and disrupts the usual anterior-posterior relationship, making true corneal refractive power difficult to determine.
Physiologically, the normal cornea usually exhibits mild positive spherical aberration (SA); myopic treatments often increase positive SA (central flattening), whereas hyperopic corrections tend to induce negative SA (central steepening with peripheral flattening).
Matching IOL asphericity to the post-refractive cornea is not simply about neutralising aberrations but about achieving the right final aberration balance for that patient. After myopic laser ablation, the cornea often carries increased positive SA. One strategy is to partially offset this with a negative-SA monofocal IOL (e.g. Tecnis or AcrySof IQ) to improve quality of vision. However, many surgeons deliberately avoid fully cancelling small amounts of positive SA because it is frequently well tolerated and can actually increase depth of focus and possibly reduce near spectacle dependence. In those cases, an aberration-neutral IOL (e.g. RayOne monofocal or several Bausch + Lomb monofocals) is often preferred to preserve some functional range rather than correcting the eye’s SA. Conversely, some lenses intentionally introduce positive SA (e.g. RayOne EMV) to extend range of focus, which can be useful when the overall optical profile and patient priorities make that trade-off acceptable [9-13].
Diagnostics: measuring the altered cornea
Axial length remains the single most critical factor in IOL accuracy, but unreliable corneal power is the main source of error postoperatively. Standard keratometry assumes a fixed refractive index (1.3375) and a constant relationship between the anterior and posterior surfaces. In addition, effective lens position (ELP) prediction can be biased because many formulas partly infer ELP from corneal power, increasing the IOL power error [14].
To prevent the underestimation of power changes common with traditional keratometry, total keratometry (TK) is essential. Newer tools use TK to measure both anterior and posterior surfaces, allowing true net corneal power to be assessed.
- Scheimpflug-based tomography (Pentacam, Orbscan, etc.) measures both anterior and posterior curvature and can generate true net power equivalent keratometric readings across multiple zones [15,16].
- Optical coherence tomography (OCT)-based biometers (including IOLMaster 700 and Heidelberg Anterion) employ swept-source technology to capture TK values that integrate both corneal surfaces [17].
- Anterior segment OCT devices like the MS-39 (CSO) combine Placido disc topography with spectral-domain OCT for highly detailed epithelial and stromal mapping [18].
Corneal astigmatism
Careful analysis using topography or tomography is required to differentiate between regular and irregular forms. Regular corneal astigmatism can often be corrected with toric IOLs; irregular astigmatism (e.g. after decentred ablations or RK) cannot be fully addressed and may favour small-aperture lenses such as the IC-8 or topography-guided laser enhancement prior to IOL surgery [5,19].
Modern calculation formulas
Historical methods are no longer the gold standard – modern formulas using TK or artificial intelligence (AI) have significantly improved outcomes.
The ASCRS post-refractive IOL calculator remains an invaluable tool, incorporating multiple methods (Barrett, Haigis-L, etc.) to provide a consensus recommendation. A European counterpart is the ESCRS IOL Calculator, which similarly aggregates modern formulas within a single interface.

Table 1: Comparison of modern IOL formulas for post-refractive eyes.
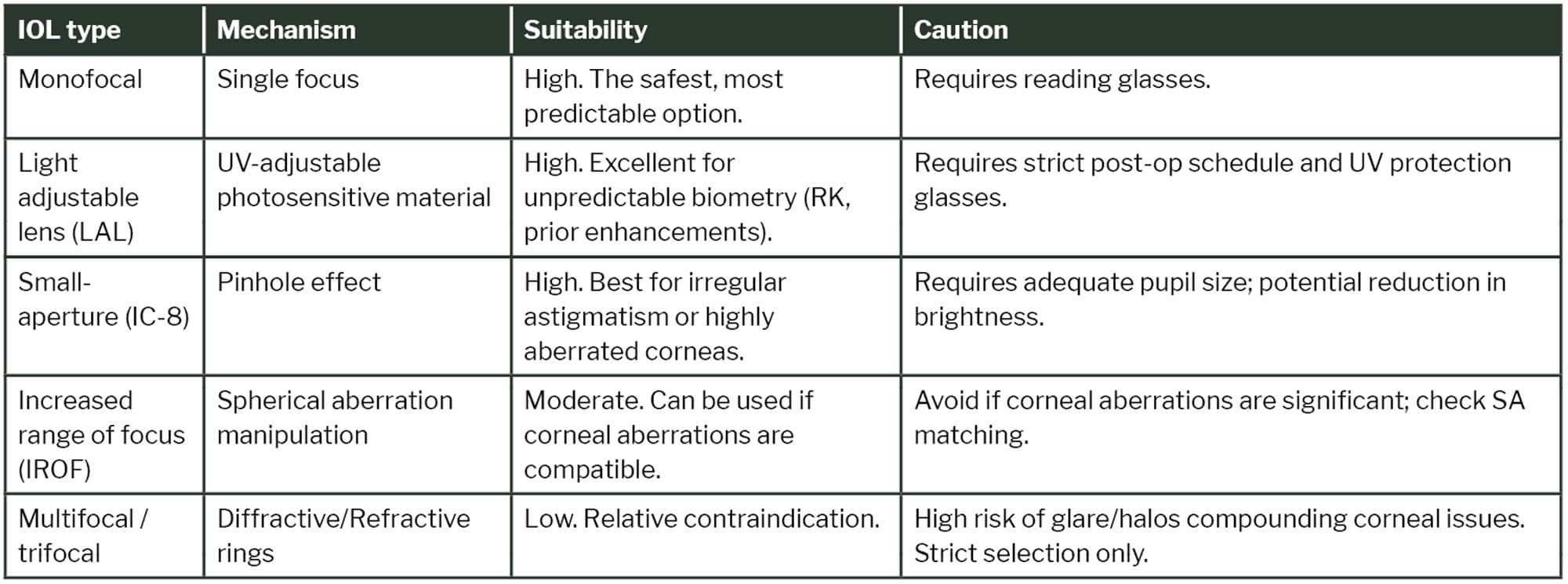
Table 2: IOL options for the post-refractive patient.
IOL choice and technology
In appropriately selecting IOLs for post-refractive eyes, optical performance is not necessarily compromised; it can be optimised for functional vision, and modest residual SA may enhance depth of focus and reduce near spectacle dependence.
Monofocal lenses remain the safest and most predictable option, providing the best contrast sensitivity with minimal optical side-effects; reading glasses are usually required unless a monovision approach is used [20,21]. Monovision targets distance in the dominant eye and mild myopia in the fellow eye to improve near function, with fewer photic phenomena than multifocal methods.
Multifocal and trifocal IOLs increase range of vision but reduce contrast sensitivity and can cause glare and halos. They are relatively contraindicated in patients with previous corneal refractive surgery because pre-existing corneal irregularities increase the risk of visual disturbances and unpredictable optical outcomes – if considered, strict patient selection and counselling are essential [9,20].
Increased range of focus (IROF) IOLs elongate the focal range with less dysphotopsia than traditional multifocals but have less robust near vision than trifocals [20]. Many manipulate SA, so care is required to avoid compounding existing corneal aberrations; aberration-neutral monofocal lenses may be preferable when the aim is to preserve useful corneal SA and functional range of focus.
Toric IOLs are effective for correcting corneal astigmatism though their performance diminishes with irregular corneae [5,22].
Innovation continues in this space. Newer diffractive designs demonstrate promising results when selection criteria are strict and residual aberrations minimal. The Rayner Galaxy is a new spiral IOL designed to deliver a continuous full range of focus with minimised dysphotopsia. While promising, early data suggests these should still be used with caution in eyes with significant higher order aberrations (HOAs) [23].
For eyes with highly irregular corneae or where biometry is uncertain (e.g. RK or decentred ablations), two technologies stand out.
- Light adjustable lenses (LALs) allow postoperative customisation. Using UV light to alter lens curvature, it enables adjustments of up to ±2D in sphere and 3D in cylinder, permitting precise refractive targeting once healing is complete. The LAL is particularly beneficial for post-LASIK, PRK and RK eyes where preoperative prediction is unreliable [24,25].
- LALs allow another IOL option that use a pinhole effect to increase depth of focus. They have been shown to reduce HOAs and are useful for irregular corneas and post-refractive surgery [26,27].
Managing expectations
Managing expectations is central to postoperative satisfaction. Preoperative questionnaires and comprehensive counselling should include the risk of refractive surprise, possible residual refractive error and/or enhancement procedures, and adaptation after multifocal implantation. For patients comfortable with glasses, monofocal IOLs (including monofocal torics) remain the most dependable and visually stable choice.
Conclusion
Cataract surgery in patients with a history of corneal refractive surgery requires an individualised approach that integrates detailed corneal imaging, advanced IOL calculation formulas and realistic patient counselling. By leveraging TK, AI-based formulas and adjustable or small-aperture IOL technologies, surgeons can now navigate the optical complexities of these eyes with greater confidence.
TAKE HOME MESSAGES
-
Understand the history: Identify whether the previous surgery was myopic (central flattening) or hyperopic (central steepening) as this dictates the SA profile.
-
Use total keratometry (TK): Standard keratometry is unreliable in these eyes. Scheimpflug, OCT-biometry or MS-39 tomography are essential for accurate corneal power measurement.
-
Formula selection: Utilise the ASCRS calculator and modern AI-driven formulas (Barrett True-K, EVO 2.0, Pearl-DGS) rather than historical methods.
-
Lens selection: Multifocals are relatively contraindicated. LAL and small-aperture IOLs are robust solutions for unpredictable or irregular corneas (e.g. RK).
-
Counsel carefully: Set realistic expectations regarding the risk of refractive surprise and the potential need for glasses or enhancement procedures.
References
1. Vanathi M. Post-laser vision correction cataract surgery: What makes it challenging? Indian J Ophthalmol 2024;72(9):1231–2.
2. Devgan U. Cataract surgery with phakic IOL removal (2018) [Online]:
https://cataractcoach.com/2018/06/07/
cataract-surgery-with-phakic-iol-removal
3. Feiz V. Intraocular lens power calculation after corneal refractive surgery. Middle East Afr J Ophthalmol 2010;17(1):63–8.
4. Gettinger K, Masui S, Omoto M, et al. Accuracy of recent intraocular lens power calculation methods in post-myopic LASIK eyes. Sci Rep 2024;14(1):26560.
5. Wang L, Koch DD. Intraocular lens power calculations in eyes with previous corneal refractive surgery. Taiwan J Ophthalmol 2021;12(1):22–31.
6. Chang V. Bunya VY, Lizárraga MT. Radial Keratotomy: Complications Management (2025) [Online]:
https://eyewiki.org/w/index.php?title=
Radial_Keratotomy:_Complications
_Management&oldid=118923
7. Turnbull AMJ. IOL calculations in eyes with a history of radial keratotomy (2021) [Online]:
https://crstodayeurope.com/articles/2021
-sept/iol-calculations-in-eyes-with-a
-history-of-radial-keratotomy
8. Al-Somali A, Muhammad Abouollo H, Al-Jindan M, et al. Corneal asphericity and its related factors. Medical hypothesis discovery and innovation in ophthalmology. Med Hypothesis Discov Innov Ophthalmol 2023;12(3):142–9.
9. Bai G, Li X, Zhang S, et al. Analysis of visual quality after multifocal intraocular lens implantation in post-LASIK cataract patients. Heliyon 2023;9(5):e15720.
10. Ang RET, Lee PL, Torres RS, et al. Higher-order aberrations and spherical aberration in various age groups after LASIK and cataract surgery. BMC Ophthalmol 2025;25(1):271.
11. Llovet-Rausell A, Navalón-Tortosa J, Druchkiv V, et al. Patient satisfaction and quality of vision after bilateral implantation of enhanced monofocal IOL and mini-monovision: a prospective study. Eye Vis (Lond) 2025;12(1):23.
12. Kozhaya K, Kenny PI, Esfandiari S, et al. Effect of spherical aberration on visual acuity and depth of focus in pseudophakic eyes. J Cataract Refract Surg 2024;50(1):24–9.
13. Nochez Y, Majzoub S, Pisella PJ. Effect of residual ocular spherical aberration on objective and subjective quality of vision in pseudophakic eyes. J Cataract Refract Surg 2011;37(6):1076–81.
14. Savini G, Hoffer KJ. Intraocular lens power calculation in eyes with previous corneal refractive surgery. Eye Vis (Lond) 2018;5:18.
15. Helaly HA, El-Hifnawy MAM, Shaheen MS, El-Kheir AFA. Accuracy of corneal power measurements for intraocular lens power calculation after myopic laser In situ Keratomileusis. Middle East Afr J Ophthalmol 2015;23(1):122–8.
16. Helaly HA, Elhady AM, Elnaggar OR. Accuracy of traditional and modern formulas for intraocular lens power calculation after radial keratotomy using standard keratometry. Clin Ophthalmol 2023;17:2589–97.
17. Blehm C, Hall B. Refractive predictability of a swept source optical coherence tomography biometer in long and short eyes implanted with extended depth of focus intraocular lenses. Clin Ophthalmol 2023;17:3525–30.
18. Khamar P, Rao K, Wadia K, et al. Advanced epithelial mapping for refractive surgery. Indian J Ophthalmol 2020;68(12):2819–30.
19. Stulting RD, Durrie DS, Potvin RJ, et al. Topography-guided refractive astigmatism outcomes: predictions comparing three different programming methods. Clin Ophthalmol 2020;14:1091–100.
20. Stephenson PD, Breyer DRH, Lücht D, et al. Monofocal, multifocal, and EDOF IOLs (2021) [Online]:
https://crstodayeurope.com/articles/
jan-2021/monofocal-multifocal-and-edof-iols
21. Brennan K. Odd couple: multifocals and post-refractive eyes. (2017) [Online]:
www.reviewofophthalmology.com/
article/odd-couple-multifocals
-and-postrefractive-eyes
22. Termote K, Schoor R Van, Krolo I, et al. Combination of a monofocal and one type of extended depth-of-focus (zonal refractive) intraocular lens (COMEDI) in bilateral cataract surgery protocol: a monocentric, randomised, parallel group trial in cataract surgery. BMJ Open Ophthalmol 2024;9(1):e001572.
23. Abela-Formanek C, Amon M, Auffarth GU, et al. Performance of the first spiral refractive intraocular lens for continuous full range of vision. J Refract Surg 2025;41(11):e1213–22.
24. Wong J, Folden D, Wandling G, et al. Visual outcomes of a second-generation, enhanced UV protected light adjustable lens in cataract patients with previous LASIK and/or PRK. Clin Ophthalmol 2023;17:3379–87.
25. Hengerer F. Use of the light adjustable lens after corneal refractive surgery (2017) [Online]:
https://crstodayeurope.com/articles/
2017-jun/use-of-the-light-adjustable
-lens-after-corneal-refractive-surgery
26. Hunter L. IOL calculations for challenging patients (2023) [Online]:
www.reviewofophthalmology.com/
article/iol-calculations-for-challenging-patients
27. Barnett V, Barsam A, Than J, Srinivasan S. Small-aperture intraocular lens combined with secondary piggyback intraocular lens during cataract surgery after previous radial keratotomy. J Cataract Refract Surg 2018;44(8):1042–5.
[All links last accessed April 2026]
Declaration of competing interests: None declared.