Myasthenia gravis (MG) is the commonest autoimmune condition to affect the neuromuscular junction. In the UK, its prevalence is 15 per 10,000 [1,2] and recent studies have shown that rates are steadily increasing [3,4].
Aims of this audit
The aim of this audit is to analyse the results of acetylcholine receptor (AChR) antibody tests performed at the Manchester Royal Eye Hospital. This is to determine the sensitivity, specificity and accuracy of the blood test, and compare it to the standards set by RSR Limited for Autoimmune Diagnostics, the company that supplies the ELISA kits used to test for AChR antibodies. They claim that the sensitivity is 92%, the specificity 99.8%.
Clinical manifestations of MG
MG presents as fatiguable skeletal muscle weakness which progressively gets worse throughout the day and is exacerbated by repetitive movements. It can be classified into subcategories based on which muscle groups are involved: ocular, skeletal / gross motor, bulbar and respiratory, with the latter two potentially life-threatening. If the symptoms exclusively affect the extraocular muscles, it is classified as ocular myasthenia gravis (OMG) which makes up 10-20% of myasthenic patients [3].
There are different theories that explain why the eye muscles are commonly targeted in MG. To maintain the position of the eye in a particular direction, extraocular muscles must sustain tonic contractions with a high frequency of neuronal firing. Also, extraocular muscles contain a lower concentration of AChRs causing them to be more vulnerable to the antibodies if present [5]. OMG can be missed in primary care due to the fluctuating nature of the symptoms, and it being mistaken for other conditions like stroke and thyroid eye disease to name a few. It can also be confused with age related ptosis and ophthalmoplegia, meaning it could be underdiagnosed in the older population. OMG can progress to generalised myasthenia gravis (GMG) within a few years if the patient is AChR-antibody seropositive, especially if they are left untreated. If the symptoms are limited to extraocular muscles for three years, it rarely develops into the generalised form (GMG) long-term [6].
Serology in myasthenia
Myasthenia is an antibody-mediated condition in which the immune system attacks post-synaptic structures. Antibodies are most commonly formed against nicotinic AChRs which are concentrated at the peaks of the synaptic fold at the neuromuscular junction [5]. Normally functioning AChRs bind to acetylcholine at two sites, allowing sodium, calcium and potassium to pass through the cell membrane. This results in cell depolarisation and muscle contraction. Acetylcholine receptors antibodies (anti-AChR) bind to the extracellular portion of the receptor and interfere with neuronal signalling [5].
The second commonest antibody found in myasthenia patients target muscle-specific kinase (anti-MuSK), a transmembrane protein that is complexed with AChR and important for its function. Although AChR antibodies are present in approximately 90% of patients with GMG it’s less common in OMG, with sensitivities ranging between 40-70% [7,8]. Its specificity is usually >90% [9]. Testing for anti-MuSK is usually second line if the patient is initially seronegative for anti-AChR. If the patient is double-seronegative (for anti-AChR and anti-MuSK), we could test for antibodies against other membrane proteins like low-density lipoprotein receptor-related protein 4 (Lrp4) and agrin, but these are less commonly done in practice [10].
Why is accurate diagnosis important for patient care?
MG is a treatable disease that has better outcomes with early intervention. Managing the condition early could prevent further complications such as myasthenic crisis, resulting in respiratory failure and the need for ventilation and intensive care admission [3].
Protocols to diagnose suspected OMG at the Manchester Royal Eye Hospital
After appropriate history taking, physical examination and orthoptic review, neuro-ophthalmology assessments should be within six weeks of referral. The following features in the history point towards a clinical diagnosis of OMG: variable ptosis, variable diplopia, fatiguability, diurnal variation, extra investigations: anti-MuSK antibodies, single fibre electromyography (SF-EMG) and successful treatment with pyridostigmine or steroids. If there is a suspicion of myasthenia, the AChR-antibody blood test is requested [7,10,11].
Thyroid function tests are routinely offered if thyroid eye disease is suspected. If a patient is seronegative with a high clinical suspicion of OMG, further tests can be carried out: anti-MuSK antibodies and SFEMG, and CT scans of the chest to investigate for the presence of a thymoma. Some patients are started on a trial of pyridostigmine if there is high clinical suspicion of OMG, and then a trial of steroids if it fails. The protocols for diagnosis and management of the different types of MG are summarised by Sussman, et al. [12]. If there were persistent doubts about a patient with negative tests, blood tests are sent to the labs in Oxford to run cellular-based assays to detect AChR antibodies.
Methods
Audit data collection
AChR-antibody tests requested at the Manchester Royal Eye Hospital are processed in the immunology labs at the Manchester Royal Infirmary via enzyme-linked immunosorbent assays (ELISA) produced by RSR Limited for Autoimmune Diagnostics. AChR-antibody test results that were requested by two consultants and one clinical fellow in the neuro-ophthalmology department from 2 April 2020 to 27 January 2022 were collected. Patient records were then accessed via the hospital’s EPR system and serology results were collected. The normal range is 0-0.44nmol/L, above which is considered a positive result. Patients were classified as being diagnosed or not diagnosed with OMG based on their clinical picture.
Patients with ambiguous test results or clinical histories were reviewed by a neuro-ophthalmology fellow and classified as having true myasthenia or not. Patient data was analysed on excel to determine the sensitivity, specificity and accuracy of the AChR-antibody test. Patients were excluded if they had intracranial tumours or orbital skull fractures.
Results
Acetylcholine receptor antibody test results
One hundred and thirty three AChR-antibody test results were collected at the Manchester Royal Eye Hospital. Nine patients were excluded for the following reasons: two had orbital floor fractures, two had intracranial tumours, four had missing patient details and one was a duplicate. One hundred and twenty-four serology results were analysed in this audit.
Patients diagnosed with OMG
Fourteen of the 124 patients (11%) were clinically diagnosed with OMG. Eleven of those patients were seropositive (true positive mean= 8.426, SD= 8.178), and four were seronegative (false negative mean= 0.345, SD= 0.098).
Patients not diagnosed with OMG
One hundred and nine of the 124 patients (87%) were not diagnosed with OMG. Eighteen of those patients were seropositive (false positives mean= 0.730, SD= 0.355) with borderline results ranging from 0.47 to 0.94, with one value slightly higher at 2.0. There were 91 seronegative results (true negative mean= 0.296, SD= 0.082).
Sensitivity and specificity
The sensitivity of AChR-antibody tests at the Manchester Royal Eye Hospital was calculated at 73%, and the tests specificity was calculated at 83%. These values have been summarised in Table 1.
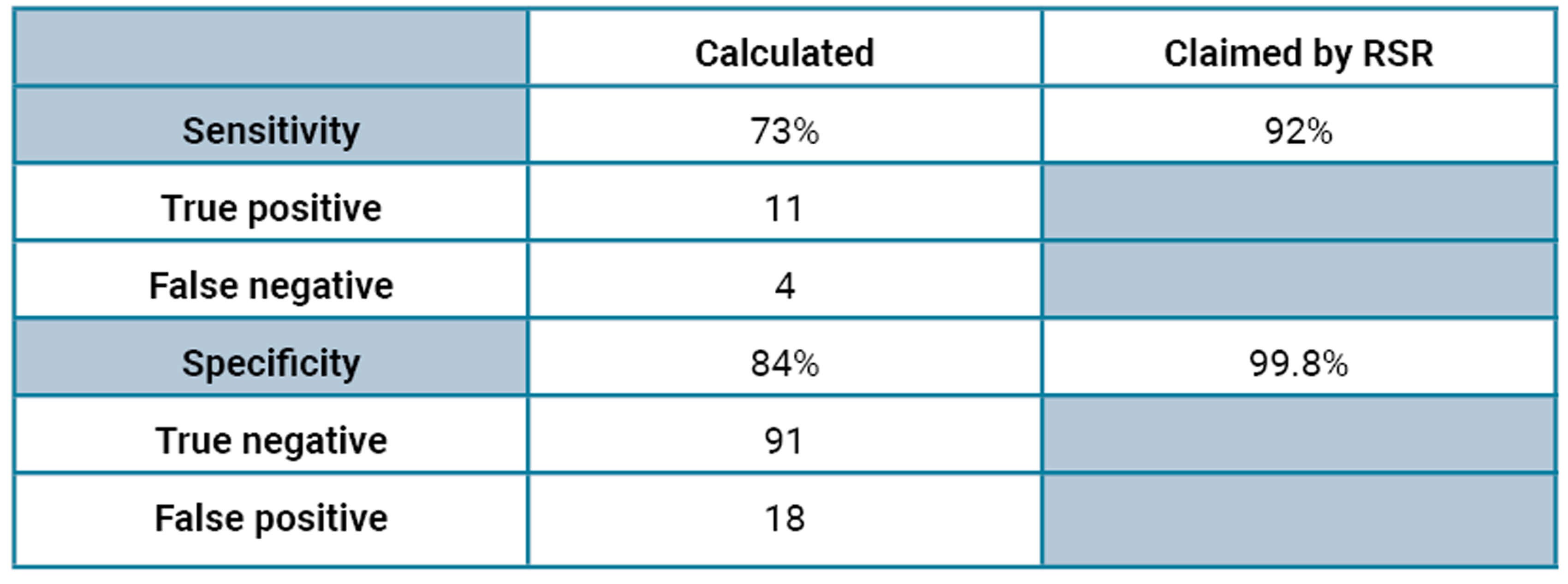
Table 1: Sensitivity and specificity of AChR-antibody tests at the Manchester
Royal Eye Hospital, along with the values needed to calculate it.
Discussion
The ELISA kits supplied by RSR Limited for Autoimmune Diagnostics used to test for AChR antibodies supposedly have a sensitivity of 92% and specificity of 99.8%. However, based on our data, the sensitivity currently lies at 73%, which is lower than that claimed by RSR, but still within the range of the 40-70% that is mentioned in the literature for ocular myasthenia [6-8]. We must keep in mind that the same kits are used to test for generalised MG, and the sensitivity of the test is usually higher for that group of patients. However, the kits claim to have 99.8% specificity, meaning that any positive test should almost certainly mean that the patient has MG.
Surprisingly, the test’s specificity was calculated at 83%, quite a difference from the claimed 99.8%, and the 91% found in the literature [9]. In fact, 62% of all positive test results were false positives (true positives n=11, false positives n=18). Most false positives were borderline ranging from 0.47 to 0.94, with one value slightly higher at 2.0. When discussing this with the neuro-ophthalmologists at the Manchester Royal Eye Hospital, they feel that the test has become unreliable when the results are borderline positive, which has resulted in multiple patients being falsely diagnosed with MG and unnecessarily treated with pyridostigmine.
After further discussion with the immunology department, they reported that when testing 48 blood samples of healthy individuals, three of the 48 results were false positives. They also informed us that other labs using the same kits have shifted their reference ranges up to 1 nmol/L, well above the 0.44 nmol/L suggested by RSR, to account for the increased rate of false positives.
Action plan moving forward
We will work with the immunology lab at the Manchester Royal Infirmary to review the reference ranges for the AChR-antibody blood tests. We will incorporate test results from the neurology department testing for MG to plot a receiver operating characteristic (ROC) curve and determine whether the cut-off point should be shifted up to increase the specificity of the test, without sacrificing its sensitivity.
Limitations
This audit is not without its limitations. Test results conducted between 29 March and 28 October 2021 were unavailable, creating gaps in the data. Also, OMG is very difficult to diagnose as it can be confused with other neurological conditions mentioned above. In addition, it is usually underdiagnosed in the elderly population.
Conclusion
In conclusion, ocular myasthenia gravis can be diagnosed with a combination of the appropriate history, examination, serology and pharmacologic investigations. OMG is diagnosed at the Manchester Royal Eye Hospital via history, examination and AChR-antibody tests as a first line investigation. Recently higher rates of false positive serology tests require further investigation, and reference ranges for the blood test should be reviewed by the immunology department.
References
1. Robertson NP, Deans J, Compston DAS. Myasthenia gravis: A population based epidemiological study in Cambridgeshire, England. J Neurol Neurosurg Psychiatry 1998;65(4):492-6.
2. Carr AS, Cardwell CR, Mccarron PO, Mcconville J. A systematic review of populartion based epidemiological studies in Myasthenia Gravis. BMC Neurol 2010;10:46.
3. Spillane J, Higham E, Kullmann DM. Myasthenia gravis. BMJ 2012;345:e8497.
4. Carey IM, Banchoff E, Nirmalananthan N, et al. Prevalence and incidence of neuromuscular conditions in the UK between 2000 and 2019: A retrospective study using primary care data. PLoS One 2021;16(12):e0261983.
5. Dresser L, Wlodarski R, Rezania K, Soliven B. Myasthenia gravis: Epidemiology, pathophysiology and clinical manifestations. J Clin Med 2021;10(11):2235.
6. Shuey NH. Ocular myasthenia gravis: a review and practical guide for clinicians. Clin Exp Optom 2022;105(2):205-13.
7. Gilhus NE, Tzartos S, Evoli A, et al. Myasthenia gravis. Nat Rev Dis Primers 2019;5(1):30.
8. O’Hare M, Doughty C. Update on Ocular Myasthenia Gravis. Semin Neurol 2019;39(06):749-60.
9. Melson AT, McClelland CM, Lee MS. Ocular myasthenia gravis: Updates on an elusive target. Curr Opin Neurol 2020;33(1):55-61.
10. Zisimopoulou P, Brenner T, Trakas N, Tzartos SJ. Serological diagnostics in myasthenia gravis based on novel assays and recently identified antigens. Autoimmun Rev 2013;12(9):924-30.
11. Lee JJ, Koh KM, Kim US. The Anti-Acetylcholine Receptor Antibody Test in Suspected Ocular Myasthenia Gravis. J Ophthalmol 2014;2014:689792.
12. Sussman J, Farrugia ME, Maddison P, et al. Myasthenia gravis: Association of British Neurologists Management Guidelines. Pract Neurol 2015;15(3):199-206.
COMMENTS ARE WELCOME





