History
An Afro-Caribbean woman, aged 30, with “scleral tattooing” for cosmetic reasons (subconjunctival dye injection), presented with bilateral upper and lower eyelid oedema for one week, and she also had restricted eye movement and blurry vision in her right eye.
- She has no other past medical history.
- On examination, firm masses were felt medially on the right upper lid, there was bilateral upper and lower lid oedema, and the conjunctiva was thickened. The right eye had restriction of depression, elevation, abduction, and adduction and the patient reported diplopia.
- There were no intraocular inflammation or fundal abnormalities present. According to a systemic inspection, nodular lesions were detected on multiple tattoos.
- Conjunctival biopsies were performed and sent for ophthalmic pathology assessment.
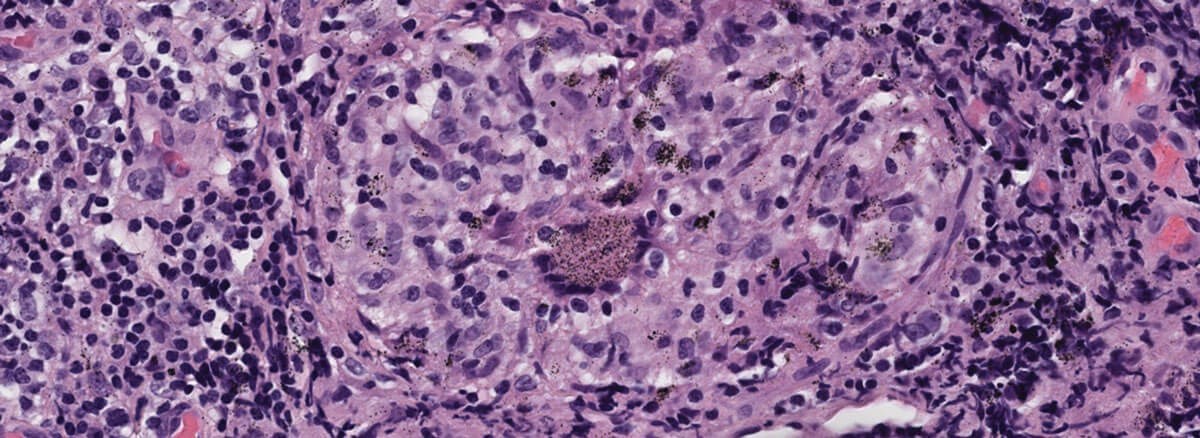
Figure 1.
Questions
- Figure 1 shows a representative H+E section of the lesion. How can this be described?
- What is the pathophysiology of granuloma formation?
- What are the differentials diagnoses?
Answers
1. This H&E stain reveals a non-caseating granulomatous inflammation with granular pigment with x40 magnification.
2. A granuloma is a small area of chronic inflammation characterised by a swarm of macrophages, which are usually accompanied by helper T-cells. Granulomas can form as a result of either a continuous T-cell response or the body’s attempt to retain a pathogen that it is unable to eradicate. Chronic inflammation may induce organ tissue damage and tissue death (i.e., necrosis) or scarring (i.e., fibrosis).
a) The pathogenic pathogen’s antigen is picked up by a macrophage and delivered to CD4+ helper T cells. CD4+ helper T cells differentiate into the TH1 subtype. As a result, TH1 cells release IL-2 and IN- γ. T-cell proliferation and macrophage activation follow, and macrophages and T-cells produce TNF-alpha, which enhances inflammatory cell accumulation.
3. Non-caseating granulomas and in particular “naked” granulomas (without a rim of lymphocytes) are the histological hallmark of sarcoidosis. Unfortunately, these are not specific, and many infectious disorders may present with granulomatous features.
a) A thorough histological examination is also essential for a correct diagnosis because some pathological signs aid in orienting a specific disease.
b) Tuberculoid granuloma with central caseous necrosis aids in the diagnosis of mycobacterial infections, cryptococcosis, histoplasmosis, and brucellosis, whereas suppurative or pyoepithelioid granulomas aid in the diagnosis of bartonellosis, yersiniosis, chlamydiosis, or tularemia.
c) Whipple’s disease granulomas, like syphilitic granulomas, typically have a sarcoid-like appearance. When a histological investigation indicates central necrosis, the kind of necrosis should be considered. Fibrinoid necrosis differs from caseous necrosis in that it has a bright red colour that marks fibrin on hematoxylin and eosin staining. This pattern is associated with vascular damage that is more typically linked to vasculitis, either immune-mediated (e.g., rheumatoid arthritis, ANCA associated-vasculitis) or infectious (e.g., rickettsiosis, syphilis).
d) The relationship between foreign body granulomatous reaction caused by tattoo dye and sarcoidosis is unknown; however, multiple accounts have revealed systemic sarcoidosis characteristics triggered by cutaneous tattooing or foreign body reactions.
COMMENTS ARE WELCOME





