History
-
A 92-year-old female patient was referred for a three-month history of a left conjunctival growth with ocular irritation.
-
Her past medical history included: hypertension, back pain and osteoarthritis, all of which were controlled by medication.
-
On examination: vision in both eyes was 6/9 aided; there was a pedunculated, non-pigmented, vascularised left caruncular lesion measuring 6x4x4mm (Figure 1); anterior segments and fundoscopy were otherwise normal.
-
A left excisional biopsy of the lesion was sent for ophthalmic pathology assessment.
-
Macroscopic examination revealed a tan fleshy nodule measuring 4mm in diameter.

Figure 1.
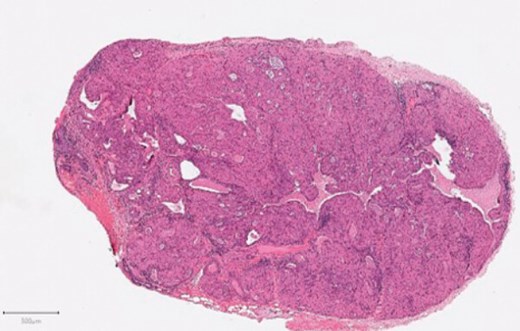
Figure 2a.
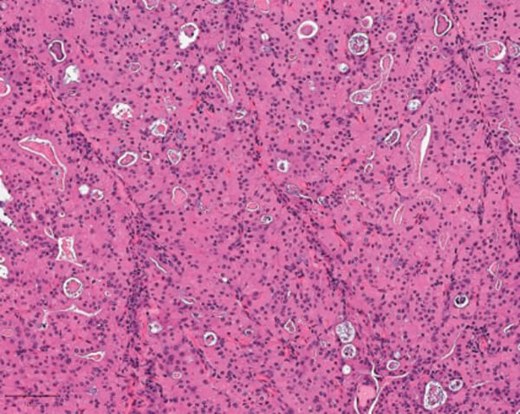
Figure 2b.
Questions
-
Figures 2a and b show representative H&E sections of the lesion. How can this be described?
-
What are the differential diagnoses?
-
What is the most likely diagnosis and what further stains may help?
Answers
1. Figure 2 shows an encapsulated lesion comprising solid nests and cords of polyhedral cells with abundant, finely granular eosinophilic cytoplasm and small, uniform round nuclei. There are scattered cystic areas containing eosinophilic secretions. There is no evidence of malignancy.
2. Differentials include: granular cell tumour (no myoepithelial cells, S100 protein positive); Warthin’s (lymphocytic background); apocrine tumours (apical snouts and decapitation secretions); and other adnexal tumours with oncocytic / apocrine changes including naevi (histomorphology of main tumour and immunohistochemistry).
3. The appearances are those of an ONCOCYTOMA, with complete excision. No further stains were necessary in this case as the histomorphological features were characteristic of oncocytoma. Ocular oncocytomas, however, demonstrate immunopositivity for cytokeratins (CK7, 8, 18 and 19); epithelial membrane antigen (EMA) and myoepithelial marker p63. Special stains: Phospho-tungstic Acid Haematoxylin (PTAH) highlight oncocytes and Periodic Acid Schiff (PAS) stain the secretions. Oncocytomas are benign tumours of secretory epithelium and can involve many organs more frequently including kidney, thyroid, parathyroid and salivary gland. Ocular oncocytomas are relatively rare, with approximately 3% of lesions arising in the carun
COMMENTS ARE WELCOME


