
Following a routine pregnancy, a newly delivered baby boy, born at term, was found to have increased work of breathing, stridor and a left medial canthal swelling. The baby required 100% oxygen via a face mask to maintain oxygen saturations. After this, the neonatal team was unable to pass an NG tube through either nostril.
Leading from this, the team first conducted a CT scan of the nasal cavity and paranasal sinuses to look for structural pathology. This demonstrated bilateral membranous choanal atresia with enlargement of both lacrimal sacs.
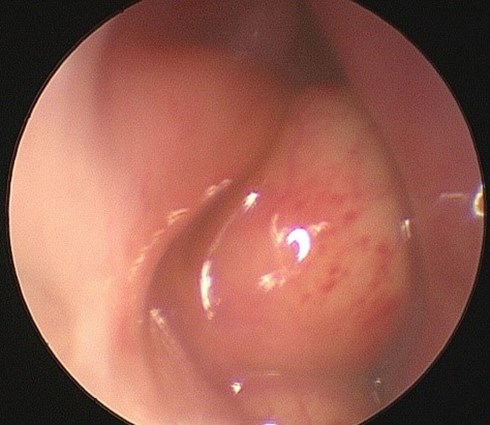
Figure 1: Nasal endoscopic photograph showing intranasal cyst beneath the inferior turbinate, due for marsupialisation.

Figure 2: Nasal endoscopic photograph showing bilateral choanal atresia and probe puncturing membrane.
The baby was taken to theatre by ENT and oculoplastics, and nasal endoscopy was performed. This confirmed the diagnosis of bilateral membranous choanal atresia and identified the presence of bilateral intranasal cysts. The child underwent membranous puncture bilaterally under ENT, followed by surgical marsupialisation of the intranasal cyst under oculoplastics. Marsupialisation of bilateral intranasal cysts beneath the inferior turbinate resulted in resolution of bilateral dacryoceles. ENT required multiple attempts at puncturing the membranous obstruction due to restenosis, as is often the case.
Discussion
Choanal atresia is a congenital abnormality whereby the patency of the communication between the nasal cavity and nasopharynx is obstructed, leading to difficulty in breathing [1]. The incidence rate of choanal atresia has been reported at 0.82 per 10,000 births [2]. In some cases, choanal atresia may be a presentation of a syndromic condition with shared ophthalmic features. Such cases include CHARGE syndrome (Coloboma of Iris or Optic nerve, Heart defects, choanal Atresia, Growth Retardation, Genital abnormalities, Ear abnormalities), with incidence estimates of 0.1-1.2 per 10,000 births [3]; and Treacher Collins syndrome (colobomas of the lateral lower eyelids, cataract, microphthalmos, atresia of lacrimal passages), with an estimated prevalence of 1 per 50,000 births [4].
Differential diagnosis for canthal swellings should be guided by their anatomical location relative to the medial canthal tendon. A swelling above the medial canthal tendon in a neonate could be an encephalocele, meningocele (or even dermoid origin or a tumour), while a swelling below the medial canthal tendon is most likely to be a dacryocele. Treatment for dacryocele is marsupialisation of the intranasal cyst, but parents should be advised to massage the patient’s lacrimal sac as this may cause spontaneous rupture of the nasal cyst by hydrostatic pressures, while awaiting marsupialisation.
Concomitant presentation of choanal atresia with intranasal cysts is rare. Importantly, however, this case highlights the need to investigate for choanal atresia, particularly in patients with a unilateral intranasal cyst, as they may first present to ophthalmology. Early liaison with ENT colleagues is encouraged, especially for patients with respiratory distress and suspected unilateral cyst to exclude an additional underlying cause of obstruction.
References
1. Hengerer AS, Brickman TM, Jeyakumar A. Choanal atresia: embryologic analysis and evolution of treatment, a 30-year experience. Laryngoscope 2008;118(5):862-6.
2. Harris J, Robert E, Kallen B. Epidemiology of Choanal Atresia With Special Reference to the CHARGE Association. Paediatrics 1997;99(3):363-7.
3. Blake KD, Prasad C. CHARGE syndrome. Orphanet J Rare Dis 2006;1:34.
4. Gorlin RJ, Cohen MM, Hennekam RCM: Syndromes of the Head and Neck. 4th ed. Oxford University Press: New York; 2001.
COMMENTS ARE WELCOME



