Syphilis has re-emerged as a significant public health concern, with the World Health Organization (WHO) estimating that 8 million adults aged 15–49 acquired syphilis in 2022. Untreated syphilis can have severe consequences, including cardiovascular, neurological and ocular complications. Ocular manifestations can occur at any stage of the disease.
Syphilis cases are rising significantly in the UK, reaching levels not seen since 1948. In 2023, there were 9513 diagnoses of infectious syphilis, a 9.4% increase from 2022, plus 3075 diagnoses of other acquired syphilis. While rates remain highest among gay, bisexual, and other men who have sex with men (GBMSM) aged 25–34, proportionally more significant increases are occurring among heterosexuals. Diagnoses are concentrated in urban areas. Increased testing rates have not kept pace with rising diagnoses, and the test positivity rate remains high, suggesting ongoing transmission.
Acute syphilitic posterior placoid chorioretinitis (ASPPC) is a rare but important manifestation of ocular syphilis, often presenting with characteristic fundus findings [1]. Early recognition and treatment prevent irreversible vision loss and systemic complications [2]. While syphilis cases have been rising globally, awareness of its varied presentations, particularly ASPPC, remains vital, especially among clinicians in emergency eye clinics. This presentation will highlight two distinct cases of ASPPC, illustrating the diverse clinical features and emphasising the importance of a high index of suspicion, appropriate investigations, and prompt management of this condition.
Case 1
A 35-year-old Caucasian man presented with a two-week history of blurred vision in both eyes, more pronounced in the left.
Six months before his presentation to the eye clinic, he was admitted for a day to the Surgical Ambulatory Care Unit (SACU) for acute abdominal pain. A CT scan of the abdomen revealed mesenteric panniculitis, mesenteric lymph node enlargement, and splenomegaly. He later developed inguinal lymph node enlargement and was placed under haematology observation. The patient identified as homosexual, with three male partners, the most recent of whom was a long-term partner of 10 years.

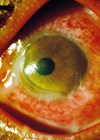
Figure 1A: Optos colour fundus photograph of the left eye at the initial visit, demonstrating a yellow placoid lesion in the macular area.

Figure 1B: Fundus autofluorescence image of both eyes at the initial visit, showing hyperautofluorescence in the macular area.

Figure 1C: OCT imaging at the initial visit revealing nodular thickening of the RPE and disruption of the EZ.
Ophthalmic examination
At the initial examination, LogMAR best-corrected visual acuity (BCVA) was 1.56 in the right eye and 0.92 (pinhole 0.68) in the left eye. A slitlamp examination revealed mild inflammation in the anterior chamber and anterior vitreous. Fundoscopy showed yellow placoid lesions in the macular area of the left eye (Figure 1A). Autofluorescence imaging demonstrated hyper-fluorescence in the macular area of both eyes (Figure 1B). OCT revealed nodular thickening of the retinal pigment epithelium (RPE) and disruption of the ellipsoid zone (EZ) (Figure 1C).
A clinical diagnosis was posterior placoid chorioretinitis with a strong suspicion of syphilis. Laboratory tests were confirmatory with positive treponema pallidum haemagglutination assay (TPHA) and a rapid plasma reagin (RPR) titre of 1:512. Human immunodeficiency virus (HIV) and toxoplasma serology were negative, leaving a final diagnosis of ASPPC.
The patient was referred to the uveitis clinic for further management. However, he repeatedly failed to attend appointments (DNA), despite multiple reminders from the nursing team and secretaries. Given the urgency of treatment, a doctor conducted a home visit to reinforce the importance of care, prompting the patient to engage with treatment.
Treatment and follow-up
Due to repeated DNAs and his medical history, the patient was admitted to the infectious diseases team for urgent treatment. He initially received oral prednisolone for three days, with IV ceftriaxone 2g twice daily initiated 24 hours after steroid commencement for two days. Treatment was then continued at home under the care of outpatient parenteral antimicrobial therapy (OPAT) team for an additional 2.5 weeks.
At the five-week follow-up, his vision improved to LogMAR 0.68 (pinhole 0.5) in the right eye and 0.9 (pinhole 0.46) in the left eye. Fundus examination revealed complete resolution of the placoid lesion in the left macular area.

Figure 1D: Optos colour fundus photograph at the six-month follow-up, showing a normal retinal appearance.

Figure 1E: Fundus autofluorescence image of both eyes at the six-month follow-up, demonstrating improvement in hyper-autofluorescence in the macular area.

Figure 1F: OCT image at the six-month follow-up, revealing complete restoration of the EZ layer and resolution of RPE nodules.
At the six-month follow-up, visual acuity improved to LogMAR 0.58 (pinhole 0.3) in the right eye and 0.4 (pinhole 0.22) in the left eye. Fundus examination appeared normal (Figure 1D), and autofluorescence imaging demonstrated significant improvement, with reduced macular hyper-fluorescence (Figure 1E). OCT showed complete restoration of the EZ layer and resolution of RPE nodules (Figure 1F).
Case 2
A 50-year-old Caucasian man presented with a two-week history of decreased vision in both eyes. His medical history included anxiety, depression, opioid dependence, recurrent deep vein thrombosis, and prior treatment for hepatitis C in 2010. He lived with his female partner but had no fixed accommodation.

Figure 2A: Optos colour fundus photography at the initial visit demonstrating regions of placoid retinal opacification involving the macula in both eyes. In the left eye, an additional large area of opacification is observed in the nasal mid-periphery of the retina.

Figure 2B: Fundus autofluorescence imaging of both eyes at the initial visit demonstrating areas of hyper-autofluorescence corresponding to the retinal lesions.

Figure 2C: OCT imaging at initial visit revealing nodular thickening of the RPE and disruption of the EZ in both eyes.
Ophthalmic examination
At the initial examination, LogMAR BCVA was 0.82 in the right eye and counting fingers in the left. The anterior segment examination was unremarkable. Fundoscopy revealed:
- Right eye: Vitritis and a macular placoid lesion extending beyond the temporal arcades (Figure 2A).
- Left eye: Mild vitritis with placoid retinal opacification involving the macula, extending beyond the temporal arcades, with an additional large area of opacification in the nasal mid-periphery (Figure 2A).
Autofluorescence imaging showed hyper-fluorescence corresponding to the retinal lesions (Figure 2B). OCT revealed nodular thickening of the RPE and disruption of the EZ (Figure 2C).
A provisional diagnosis of posterior placoid chorioretinitis was made, and the patient was sent for urgent blood tests. However, he left the clinic without providing a sample. He subsequently missed his next two appointments and returned to the eye clinic 10 days later when we could do the laboratory tests. Treponema pallidum haemagglutination assay and RPR were positive, RPR titre being 1.256. Toxoplasma IgM / IgG came back negative, confirming this as ASPPC.

Figure 2D: Optos colour fundus photography at four-week follow-up revealing spontaneous resolution of the placoid lesions from both eyes.

Figure 2E: Fundus autofluorescence image showing persistent hyper-autofluorescence with no significant changes compared to baseline visit.
Treatment and follow-up
The patient was urgently referred to the genitourinary (GUM) clinic but did not attend, citing symptom improvement and transportation difficulties. He was counselled again and provided with bus route information to facilitate attendance.Four weeks later, a fundus examination revealed the spontaneous resolution of the fundal lesions (Figure 2D); however, autofluorescence imaging showed persistent hyper autofluorescence with no significant change (Figure 2E). He later attended the GUM clinic but has not returned for his scheduled eye appointments.
Discussion
Acute syphilitic posterior placoid chorioretinitis is a pathognomonic manifestation of ocular syphilis, first described in 1990. It typically presents as yellowish, roundish, placoid lesions in the posterior pole or mid-periphery of the fundus at the level of the RPE. These lesions can coalesce into large confluent patches. It is characterised by a ground glass pattern easily differentiated from the typical whitish necrotic lesions of both herpes and toxoplasma gondi. Acute syphilitic posterior placoid chorioretinitis may also be associated with vitreous inflammation, haemorrhages, retinal vasculitis, disc oedema, and serous detachment of the RPE.
The pathophysiology of ASPPC remains unclear. Gass, et al. postulated that it involves an inflammatory reaction at the choriocapillaris-RPE-photoreceptor complex [3].
Differential diagnosis of chorioretinitis
The differential diagnosis of chorioretinitis due to cytomegalovirus, acute retinal necrosis, and toxoplasmosis relies on key clinical signs, including the presence or absence of retinal necrosis, as well as the size, shape, orientation, opacity, thickness and confluency of lesions. Additional distinguishing features include lesion colour and border characteristics. Associated inflammatory findings such as arteriolar or venular sheathing, vascular occlusion,frosted branch angiitis, and vitreous and anterior chamber inflammation severity are also crucial for assessment [4].
Multimodal imaging in ASPPC
Spectral domain (OCT) is the gold standard for assessing and diagnosing ASPPC. The clinical hallmarks include an intact external limiting membrane (ELM), a disrupted EZ, and a thickened, granular, hyperreflective RPE with nodular elevations [1]. Pichi, et al. reported transient subretinal fluid and hyperreflective spots in the choroid during the acute phase of the disease [5]. Fundus autofluorescence typically shows marked hyper autofluorescence, whereas fundus fluorescein angiography and indocyanine green angiography demonstrate hypo autofluorescence in the affected area.
British Association for Sexual Health and HIV (BASHH) guidelines
The 2024 BASHH UK guidelines for syphilis management recommend benzathine penicillin with lidocaine as the preferred treatment, now officially licensed. Ceftriaxone is an alternative option suitable in most cases where penicillin cannot be used [6].
In our first patient, systemic penicillin treatment led to the complete restoration of the ellipsoid layer and the normalisation of the RPE on SD-OCT, improving visual acuity.The second patient has DNA after receiving treatment.
Factors driving the resurgence of syphilis
Syphilis is resurging in the UK due to changing sexual behaviours, including declining condom use [7], online dating, recreational drug use, and multiple partners – especially among MSM [8]: limited screening, healthcare access, and stigma delay diagnosis and treatment, fuelling transmission. Rising infections among young adults and high HIV coinfection rates further exacerbate the issue. Tackling this requires improved prevention, expanded testing, and targeted public health strategies.
TAKE HOME MESSAGES
-
Syphilis should always be considered in patients presenting with posterior uveitis and treated quickly as neurosyphilis.
-
High DNA rates and noncompliance are common; take proactive measures at the first patient interaction, such as obtaining a blood sample and considering directly observed therapy to improve adherence.
-
Partner notification should be discussed at the time of diagnosis by a trained healthcare professional for all patients diagnosed with syphilis.
-
Patients with early, infectious syphilis should abstain from sexual contact until all lesions (if present) have resolved or until two weeks after completing treatment.
-
The spontaneous resolution of macular placoid lesions due to ASPPC does not indicate disease resolution; active treatment remains necessary per BASHH guidelines.
References
1. Neri P, Pichi F. Acute syphilitic posterior placoid chorioretinitis: when the great mimicker cannot pretend any more; new insight of an old acquaintance. J Ophthalmic Inflamm Infect 2022;12(1):9.
2. Casalino G, Erba S, Sivagnanavel V, et al. Spontaneous resolution of acute syphilitic posterior placoid chorioretinitis: reappraisal of the literature and pathogenetic insights. GMS Ophthalmol Cases 2020;10:Doc26.
3. Gass JDM, Braunstein RA, Chenoweth RG. Acute Syphilitic Posterior Placoid Chorioretinitis. Ophthalmology 1990;97(10):1288–97.
4. Davis JL. Diagnostic dilemmas in retinitis and endophthalmitis. Eye (Lond) 2011;26(2):194–201.
5. Pichi F, Ciardella AP, Cunningham ET, et al. Spectral domain optical coherence tomography findings in patients with acute syphilitic posterior placoid chorioretinopathy. Retina 2014;34(2):373–84.
6. Kingston M, Apea V, Evans C, et al. BASHH UK guidelines for the management of syphilis 2024. Int J STD & AIDS 2024;35(14):1142–60.
7.Klassen BJ, Fulcher K, Chown SA, et al. Condoms are … like public transit. It’s something you want everyone else to take: Perceptions and use of condoms among HIV negative gay men in Vancouver, Canada in the era of biomedical and seroadaptive prevention. BMC Public Health 2019;19:120.
8. Zheng Y, Ye K, Ying M, et al. Syphilis epidemic among men who have sex with men: A global systematic review and meta-analysis of prevalence, incidence, and associated factors. J Glob Health 2024;14:04004.
Declaration of competing interests: None declared.