Patients with myelodysplastic syndromes can develop transfusion-related iron overload as they become dependent on recurrent blood transfusions [1]. Iron chelation therapy is indicated for the treatment of iron overload and one established example of this is deferoxamine. However, deferoxamine ocular toxicity is a known and significant side effect.
Case Report
A 72-year-old gentleman was referred to a tertiary eye hospital by his optician due to bilateral pigmentary changes seen on his macula. He has a background of myelodysplastic syndrome, and he recently underwent iron chelation therapy with deferoxamine for transfusion-related iron overload.
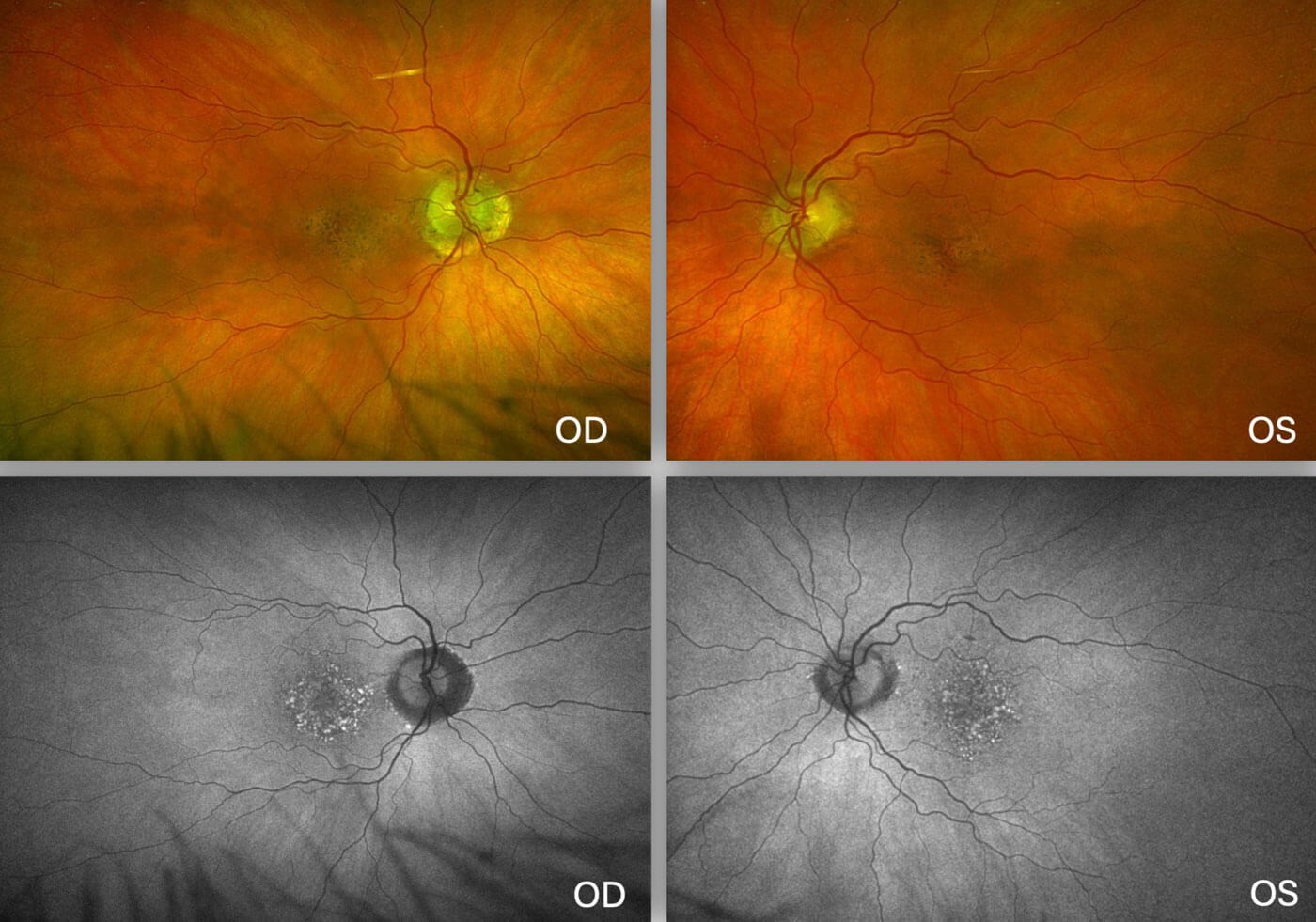
Figure 1: Colour fundus photographs (above) and fundus autofluorescence
(below) of the patient’s retinas with deferoxamine ocular toxicity.
The patient described a three-week history of changes in colour vision. On examination, his vision was 6/9 in both eyes and his colour vision was normal. Anterior segment examination showed quiet white eyes with no evidence of inflammation. Fundus examination showed no vitritis but bilateral confluent hypopigmented lesions in the macula, which appeared hyperfluorescent on fundus autofluorescence (FAF) (Figure 1). Optical coherence tomography (OCT) showed bilateral parafoveal flecks and multiple confluent hyperreflective deposits in the retinal pigmentary epithelium (RPE) (Figure 2). These findings were suspicious of deferoxamine toxicity, so he was referred for electrodiagnostic testing (EDT).
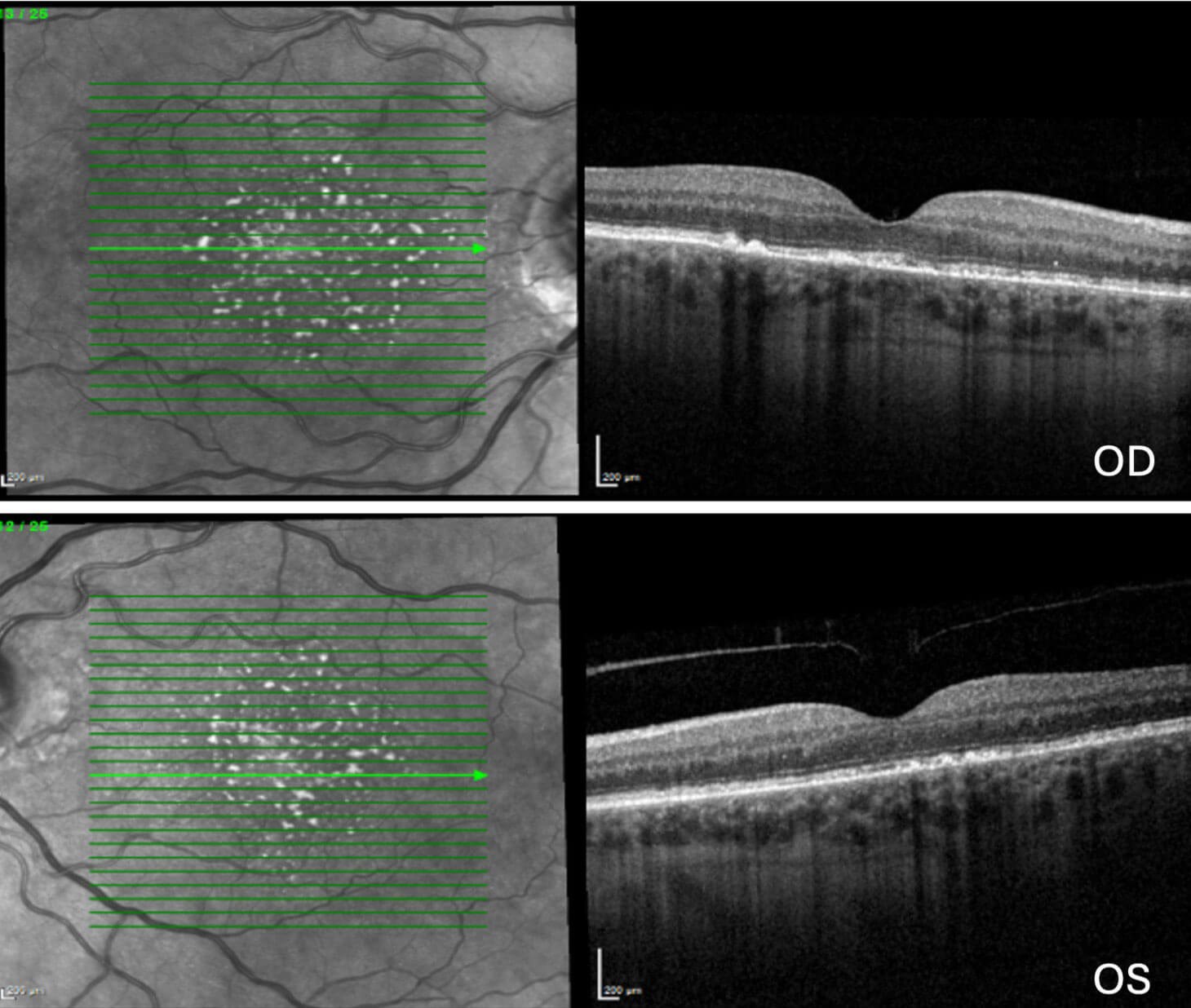
Figure 2: OCT scan of the patient’s maculas with deferoxamine ocular toxicity.
His electrooculogram (EOG) readings were 200% in both eyes, and full-field electroretinogram (ERG) revealed normal rod and cone responses. However, his pattern ERG results were reduced bilaterally. Overall, EDT findings were consistent with a bilateral maculopathy.
Although his normal EOG was not typical of deferoxamine toxicity, the amalgamation of his fundus appearance, FAF, OCT images, and pattern ERG findings were consistent with deferoxamine ocular toxicity. The patient is continuing to be monitored by the medical retina team and haematology was advised to avoid deferoxamine in his future management.
Discussion
Although deferoxamine is an important iron chelating agent listed in treatment guidelines, it is associated with a wide range of side effects. Ocular symptoms of deferoxamine toxicity include reduced visual acuity, night blindness, colour-vision defects and visual field defects. These symptoms arise as deferoxamine directly causes cell death in RPE cells via the activation of p38 pathway [2].
Fundus examination classically reveals characteristic macular pigmentary changes or pigmentary mottling in equatorial RPE [3]. In the earlier stages of retinopathy, OCT resembles basal laminar drusen, appearing as focal bumps in the RPE. In established disease, OCT shows loss of the ellipsoid zone as well as hyperreflective dome-shaped deposits at the level of the RPE.
Fundus autofluorescence is particularly useful in investigating deferoxamine retinopathy because it depicts the health and functioning of the RPE. Four phenotypic patterns were described in patients on long-term deferoxamine treatment: minimal change (small spots <100microns), focal (at least one medium sized spot between 100–200microns), patchy (at least one large area >200microns), and speckled (RPE changes extending beyond the macula) [4]. Interestingly, a 20-month follow-up on these patients showed different disease courses depending on the FAF pattern they had. In cases where deferoxamine treatment was continued, patients with minimal change showed only slight enlargement of the affected areas while patients with focal pattern had insignificant FAF changes [4]. However, patients with patchy or speckled pattern experienced progressively large areas of RPE atrophy, leading eventually to loss of vision [4]. Using FAF to identify the type of deferoxamine retinopathy the patient has can help better inform clinicians when weighing up the risks and benefits of continuing deferoxamine therapy.
Electrodiagnostic testing aids the diagnosis of deferoxamine toxicity as they identify retinal functional abnormalities [4]. In deferoxamine toxicity, the main abnormality typically lies in the pattern ERG results, while EOG and full-field ERG results are often only slightly reduced [4]. These tests have shown to be a good indicator of the disease and may reveal a higher level of retinopathy than is seen on fundus exam.
Case studies have reported differing conclusions on the reversibility of deferoxamine retinopathy, ranging from recovery of visual deficits to permanent visual changes even after discontinuing the medication. However, it is generally advised for patients to discontinue deferoxamine therapy if they develop ocular toxicity, to prevent further RPE damage and subsequent deterioration of their vision [3].
Deferoxamine is still widely prescribed in the management of transfusion-related overload, so ophthalmologists should be familiar with the investigation modalities best suited to identify early changes and to confirm diagnosis of deferoxamine ocular toxicity.
References
1. Gattermann, N. Iron overload in myelodysplastic syndromes (MDS). Int J Hematol 2018;107:55–63.
2. Klettner A, Koinzer S, Waetzig V, et al. Deferoxamine mesylate is toxic for retinal pigment epithelium cells in vitro, and its toxicity is mediated by p38. Cutan Ocul Toxicol 2010;29(2):122–9.
3. Haimovici R, D’Amico DJ, Gragoudas ES, et al. The expanded clinical spectrum of deferoxamine retinopathy. Ophthalmology 2002;109(1):164–71.
4. Di Nicola M, Barteselli G, Dell’Arti L, et al. Functional and Structural Abnormalities in Deferoxamine Retinopathy: A Review of the Literature. Biomed Res Int 2015:2015:249617.
Declaration of competing interests: None declared.






