Anisocoria means the presence of difference in the size of the right and left pupils. It is a sign of an abnormality in the efferent pathway. The first question facing the ophthalmologist is to ascertain if anisocoria is present or not. The second question to answer is which pupil is the defective one.
Question 1: is there anisocoria?
Look at both pupils in ambient room light conditions and measure size of the pupil in each eye. It is also important to note any obvious abnormalities in the shape of the pupil. Having ascertained the presence of anisocoria, the ophthalmologist needs to answer the next question: which is the abnormal pupil?
Question 2: is the smaller or the larger pupil abnormal?
In order to answer this question, pupil size needs to be measured in different light conditions by changing the level of light in the examination room.

Figure 1: Horner’s Syndrome in the right eye. Note the subtle upper lid ptosis and anisocoria
with right pupil smaller than the left. This was made more prominent in dark conditions.
Anisocoria more in darkness
- Physiological anisocoria: the difference in size is usually 0.5-1.0mm, the difference is usually similar in light and dark conditions but could be a bit more obvious in dark conditions. It is estimated that up to 20% of the population will have some form of anisocoria. Looking at old photos could help with the diagnosis.
- Inhibition of the sympathetic pathway (Horner’s syndrome) – Figure 1: features of this include miosis, subtle ptosis, lower lid reverse ptosis, apparent enophthalmos, dilation lag and anhidrosis. Other features include iris depigmentation in congenital cases. Various pharmacological agents could be used to confirm the diagnosis and try to localise the site of the lesion. Cocaine dilates the normal pupil but not the affected pupil so it increases the anisocoria. Hydroxyamphetamine can be used to localise the lesion causing Horner’s syndrome. Putting this agent into a central or preganglionic Horner’s will cause pupil dilation, however, using this agent in a postganglionic Horner’s pupil will not change the size of the pupil. Due to difficulties in access to these agents, ophthalmologists could use Apraclonidine (Iopidine) to confirm Horner’s syndrome. The pupil develops hypersensitivity (after three to seven days) and installing Iopidine into both eyes will cause reversal of anisocoria as the affected pupil will dilate compared to the normal pupil. It does not localise the lesion. Due to that, most acquired Horner’s syndrome pupils will need neuro imaging to the whole sympathetic chain to rule out compressive lesions or carotid dissection.
- Sympathetic hypersensitivity: this could manifest itself as benign episodic unilateral dilation (usually in young migraine sufferers), tadpole pupil, and whiplash injury (causing unilateral sympathetic irritation). This also could be caused by pharmacological stimulation to pupil dilator muscle in one eye. Examples include cocaine, eye whitening drops and some pulmonary treatment agents.
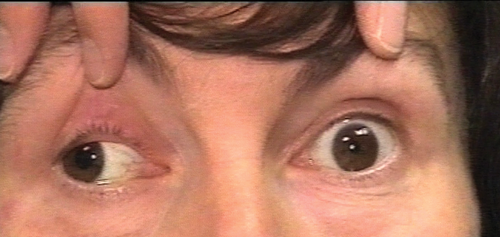
Figure 2: Oculomotor cranial nerve palsy. The patient had right ptosis
(needed to be lifted to assess motility and pupils), exotropia and right pupil larger than the left.
Anisocoria more in light
Inhibition of the parasympathetic pathway: depending on the site of the lesion, this could cause an isolated dilated pupil, a combination of iridoplegia and cycloplegia (internal ophthalmoplegia) or internal and external ophthalmoplegia (oculomotor palsy).
- Tonic pupil: this is caused by damage to the ciliary ganglion or short ciliary nerves. Features include light – near dissociation, tonic near response, parasympathetic hypersensitivity and focal iris paralysis (vermiform movements). The cause of this nerve damage could be localised to the eye and the orbit or part of widespread neuropathy. Holmes – Adie pupil is a subcategory of the tonic pupil.
- Oculomotor nerve palsy – Figure 2: this would cause various external ophthalmoplegic features depending on the extraocular muscles affected. This includes reduced adduction, elevation, depression and possible ptosis. Most of these patients would have diplopia. It is imperative to assess these patients with full orthoptic assessment and if third nerve palsy is suspected, urgent neuroimaging is necessary especially to rule out aneurysms.
- Damage to the iris sphincter: surgical or traumatic, this could be examined on the slit-lamp.
- Pharmacological dilation of the pupil: this usually fails to constrict to pilocarpine 1%.
Conclusion
In practical terms, when faced with anisocoria, ophthalmologists need to confirm the finding by measuring pupil size in each eye in ambient room light. Then the pupils need to be measured in different light conditions (dark and bright light). It is also important to note any other obvious features such as ptosis.
If the anisocoria is worse in darkness then it is usually the small pupil not dilating and it is important to rule out or confirm Horner’s syndrome using Iopidine 1% then arrange relevant neuroimaging. If the anisocoria is worse in light then it is usually the large pupil not constricting and it is important to rule out third cranial nerve palsy by assessing ocular motility.

Figure 3: Our algorithm for assesing and investigating anisocoria.
Other conditions such as Adie’s pupil, physiological anisocoria and benign episodic pupil dilation pose less of risk if not diagnosed instantly. The algorithm (Figure 3) shows our approach to assessing and investigating anisocoria.
Further reading
1. Miller N, Newman NJ, Biousse V, Kerrison JB: Walsh and Hoyt’s Clinical Neuro-Ophthalmology: The Essentials. 2nd edition. Lippincott Williams and Wilkins; 2008:299-315.
2. Kline LB: Neuro-Ophthalmology – Review Manual. 6th edition. Slack Inc; 2007:125-37.
3. Gross JR, McClelland CM, Lee MS. An approach to anisocoria. Curr Opin Ophthalmol 2016;27(6):486-92.
COMMENTS ARE WELCOME


