- Sponsored Content -
Better data, smarter commissioning, and genuine collaboration can help prevent avoidable sight loss, says a new report commissioned by ophthalmology provider Newmedica
What are the risks of ophthalmology follow-up delays for patients?
Follow-up care is where eye conditions such as glaucoma and age-related macular degeneration (AMD) are actively managed over time. Patients are no longer being assessed - they are being treated, monitored and stabilised.
When delays occur here, the consequences are different. They are not about waiting longer for diagnosis - they are about preventable deterioration. Patients on follow-up waiting lists face a ninefold risk of avoidable sight loss compared with new patients.

Nigel Kirkpatrick.
‘Hidden delays in follow-up care are risking avoidable clinical risk. Patients risk being lost in the system at a point where timely monitoring is essential to preserving sight,’ says Nigel Kirkpatrick, consultant ophthalmologist and medical director at Newmedica.
What does the data tell us?
The report highlights how in England around one in 12 patients awaiting first appointments for specialist treatment are in ophthalmology.
More than 11.4 million people are awaiting follow-up care across all specialities, yet there is no requirement to record and publish data on follow-up waiting times. The lack of transparency is leading to patients being ‘lost in the system’ and facing deteriorating health due to long delays.
At the same time, analysis in the report shows waiting list pressure increasing across many integrated care boards (ICBs) during 2025, indicating that patient need continues to outstrip available treatment capacity. ICBs commission regional NHS services in England.
What about patient choice?
Patient choice refers to the legal right of patients in England to choose their healthcare provider at the point of referral.
‘We are seeing a structural blind spot in how data is captured and used. If follow-up delays are not visible, the concern is that they are not prioritised. That has direct risks for patient outcomes,’ explains Mr Kirkpatrick.
‘Patients and commissioners need clear visibility of this data. It would empower patients to be able to make more informed decisions about their care. For health commissioners, they can plan effective services informed by data to meet patient need for wet AMD and glaucoma for example.’

What is the capacity within the system?
Capacity exists - but it is not always used effectively.
‘Capacity exists across both NHS and independent providers,’ says Mr Kirkpatrick. ‘But it is not consistently commissioned in line with patient need - limiting access to care and increasing clinical risk.
‘The system must make better use of all high-quality capacity available to it – including expert optometrists.’
He adds that Newmedica is also committed to developing the ophthalmology workforce to support capacity with expertise – including placements for doctors in training. There are also placements and CPD for community optometrists alongside upskilling wider teams at Newmedica.
The report further highlights how Selective Laser Trabeculoplasty (SLT) is a laser treatment recommended by NICE for early glaucoma. The expectation is that SLT should be routinely offered as a first line treatment for chronic open angle glaucoma and ocular hypertension, alongside drops.
‘Throughout the independent sector, SLT is now embedded within modern glaucoma pathways,’ says Mr Kirkpatrick.
SLT uses short pulses of light to improve the eye’s fluid drainage, lowering pressure safely and effectively. Many patients can avoid or reduce the need for daily eye drops, hence SLT treatment can reduce long-term prescribing and follow-up costs for the NHS.
Collaboration with community optometry
‘The system performs best when each part of the pathway is working in alignment,’ notes Mr Kirkpatrick. ‘That means effective collaboration between community optometry, hospital services and independent providers to meet patient need.’
He continues: ‘Independent ophthalmology providers, working in close partnership with community optometrists, are ready to play a key role in the solution - supporting more integrated pathways that bring diagnosis and treatment closer to home while easing pressure on NHS hospital services.

The report also notes how in Wales and Scotland, shared care glaucoma services have for example been commissioned across every health board - supported by investment in upskilling primary care optometrists.
‘We could scale these types of safe, efficient services to meet demand in England with commissioning that supports higher qualifications and equipment for primary care optometrists and full IT interoperability.’
Taking this sight-saving message to parliament
The report, launched in the Houses of Parliament on 15 July, highlights how a lack of transparency over waiting times - particularly for follow-up care - is creating avoidable clinical risk as demand rises and NHS capacity remains constrained.
The event brought MPs, peers and clinicians to share practical solutions and discuss what better care could look like. It explored how ophthalmology services are commissioned across England – and how those decisions shape patient demand, access, outcomes and waiting times.
Critically, it highlighted the importance of aligning services with real patient need and reducing regional variation.
‘As eye health and patient champions, Newmedica is taking this report to the heart of government because of this hidden risk to patients,’ says Nigel Kirkpatrick, consultant ophthalmologist and medical director at Newmedica.
‘The good news is that there are steps that can be taken now by government and commissioners to prevent avoidable sight loss. As set out in the report, these include improving transparency, data-driven commissioning and enabling genuine patient choice as well making more effective use of existing capacity within the NHS and the independent sector.’
Going the extra mile for patients
Mr Kirkpatrick concludes, saying: ‘Newmedica is committed to going the extra mile for patients and the communities that we serve. The parliamentary launch of the event is part of this commitment.
‘We’ll also continue to share the report’s key messages as we maintain engagement with politicians and policymakers. Together, we can work to prevent avoidable sight loss.’
What needs to change to prevent avoidable sight loss
Newmedica is calling on politicians and policymakers to make patient choice a reality by equipping commissioners with the data, flexibility and incentives to commission high-quality care wherever it exists. It is also calling for practical steps.
-
Mandatory publication of waiting times, including follow-up care
-
Consistent commissioning of NICE-recommended treatments
-
Full IT interoperability across providers
To read the report go to www.newmedica.co.uk/championing-eye-health
More about Newmedica
We provide specialist eyecare that focuses on protecting people’s sight through the treatment of advanced eye conditions.
We care for more than 306,000 patients a year in more than 30 locations across England, working with the NHS, as well as local GPs and community optometrists, to help treat and manage a range of advanced eye conditions in local communities – and taking some of the pressure off busy waiting lists.
Founded over a decade ago by a patient and a leading eye consultant, we’ve built our services based on personal experience. That’s why we always start with patients' needs first and make sure that patients are taken care of with total understanding and compassion.
Find out more about Newmedica at newmedica.co.uk
England’s blind spots
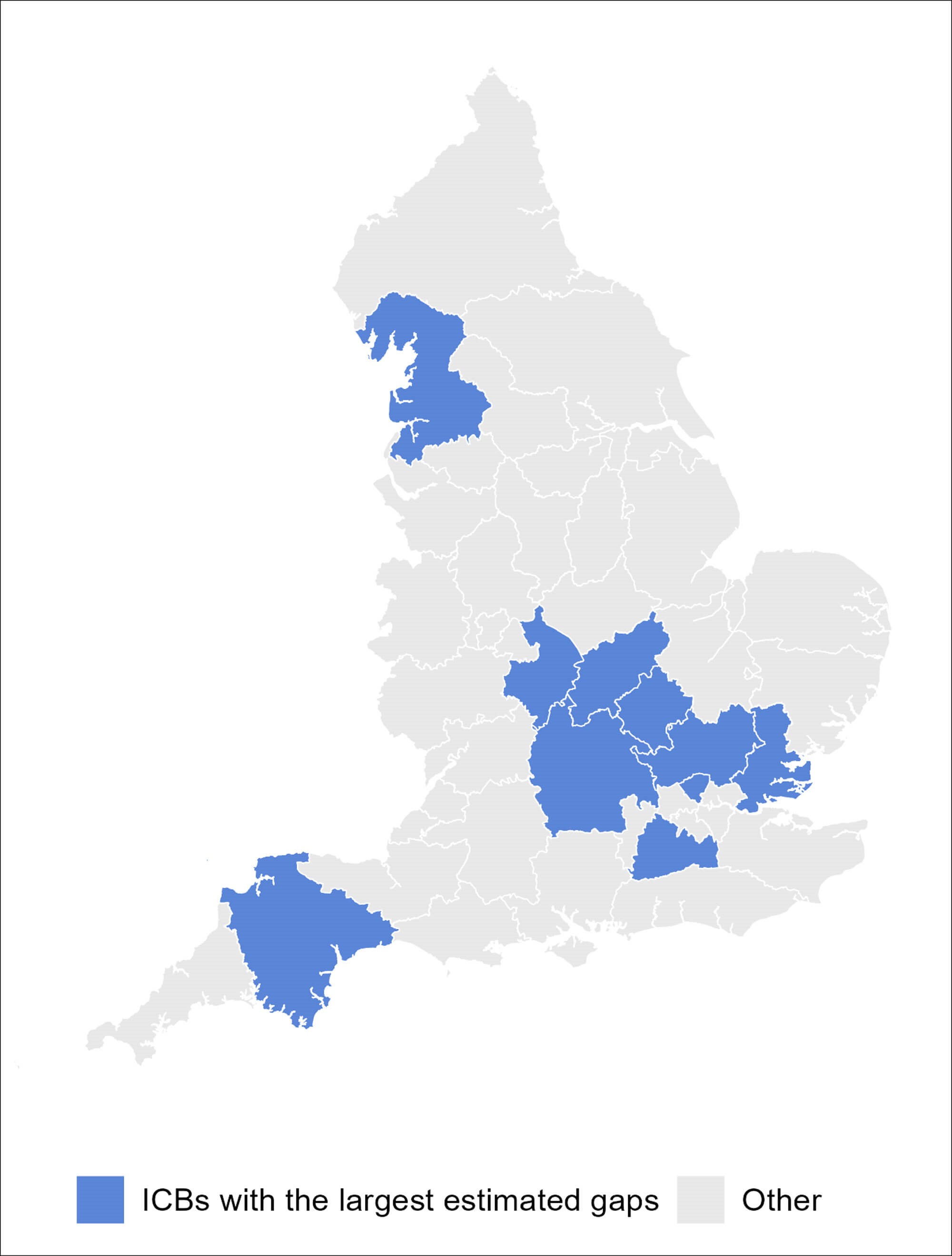
Against a backdrop of patients struggling to access eyecare and a system overwhelmed by rising demand, Newmedica commissioned Cambridge Economics Policy Associates (CEPA) to investigate eyecare waiting lists and relative ICB level ‘gaps’ between age-adjusted prevalence of serious eye conditions and treatment delivered.
Five eye care metrics for wet AMD, glaucoma, cataract, overall outpatient activity and overall eye care burden were developed. Analysis used publicly available data including prevalence estimates from the UK Eye Care Data Hub and was undertaken using ICB boundaries before April 2026. Pressure on waiting lists show 10–30% growth across many ICBs.
Using NHS Referral to Treatment data, pressures on waiting lists for eye care - as measured by additional referrals relative to completes pathways - have risen for most of ICBs during 2025. This measure is used as headline waiting list totals may mask pressures if patients are removed via re coding. It indicates that demand for care is outstripping the availability of treatment.
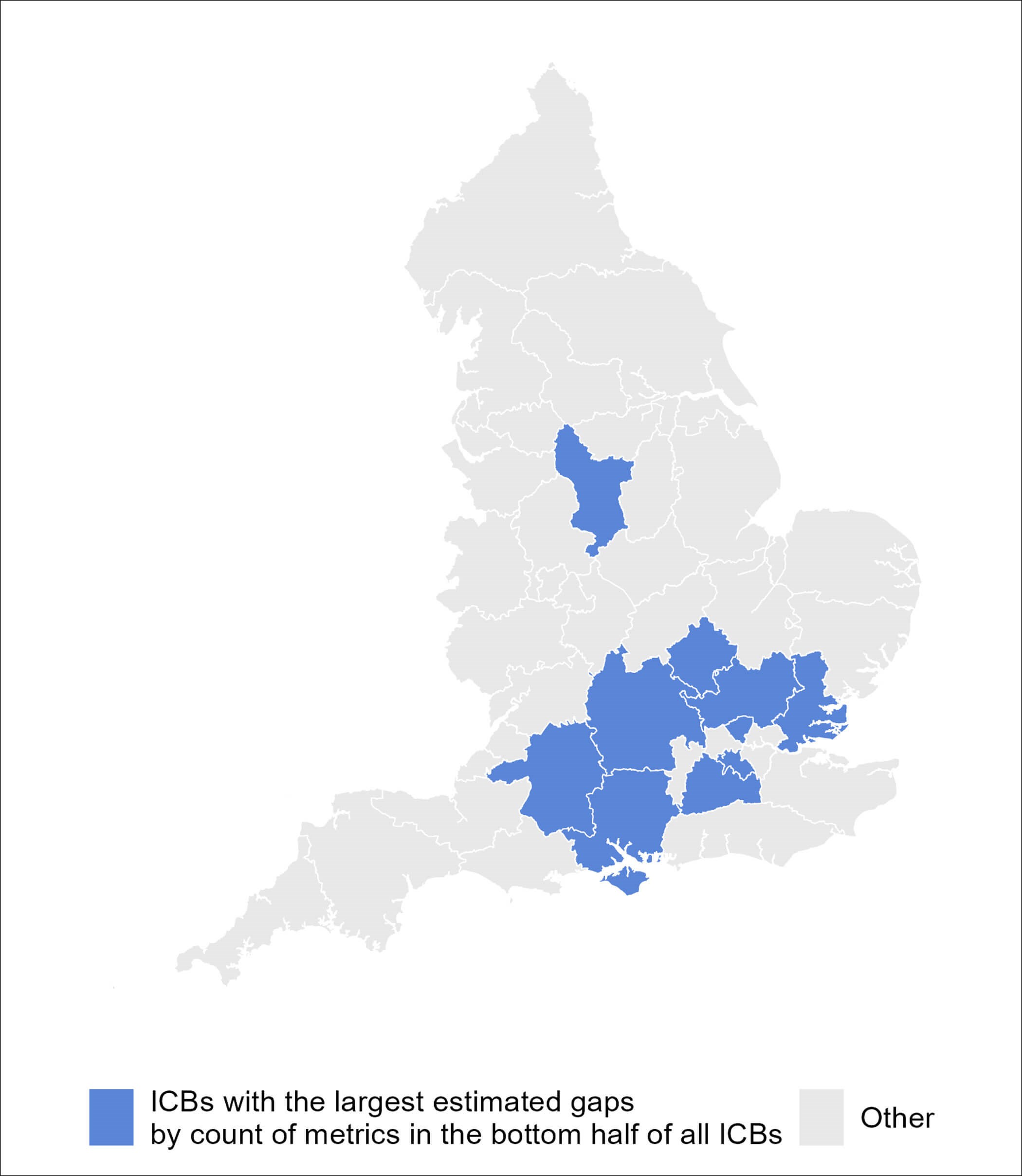
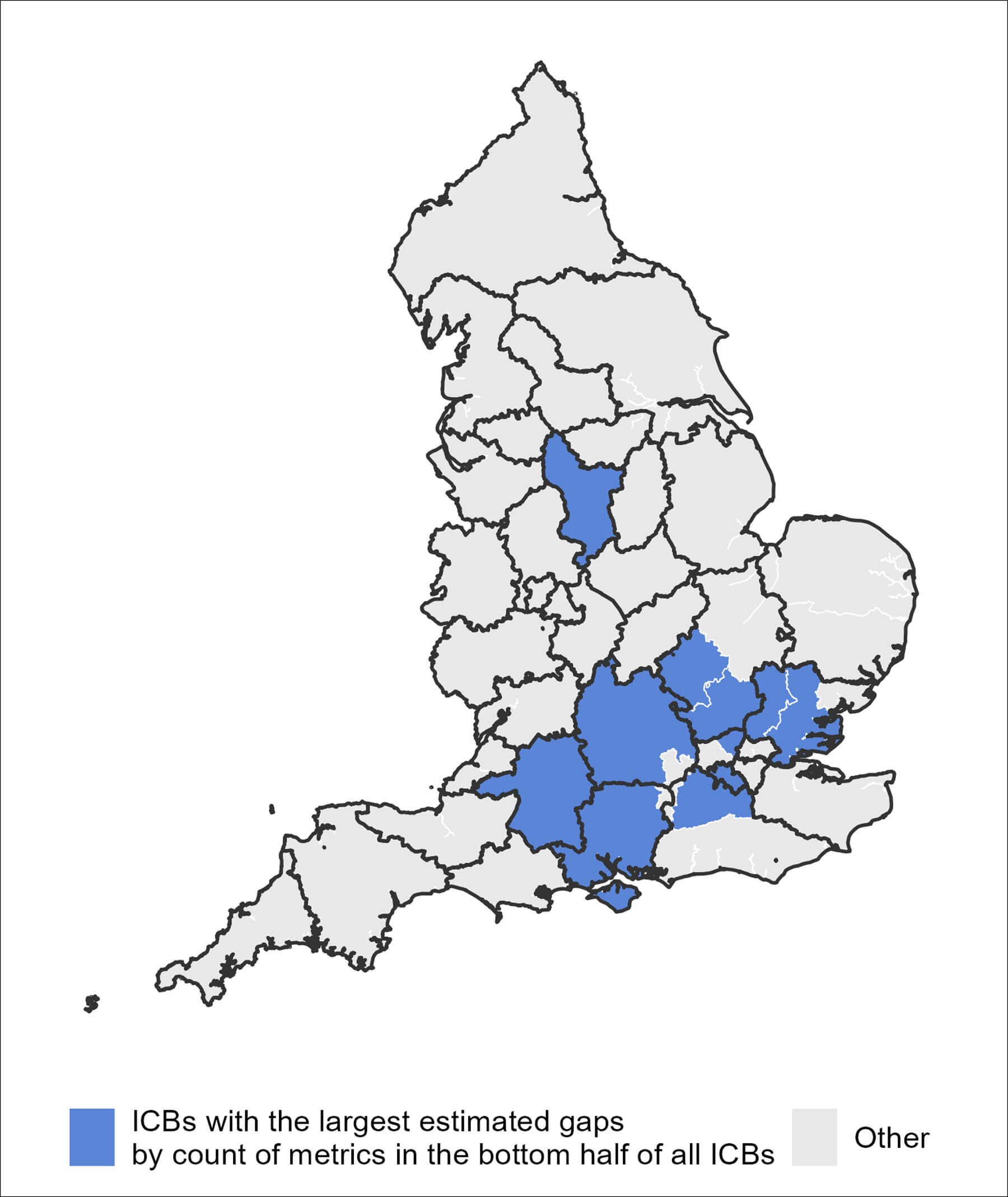
When the five metrics are combined, many of the ICBs with the greatest gap between prevalence estimates and treatment rates cluster around London and the South East. Three ICBs are ranked in the bottom half of ICBs for all five metrics: Surrey Heartlands; Buckinghamshire, Oxfordshire and Berkshire West; and Mid and South Essex.