Dry eye disease (DED) is a heterogenous condition that arises from various aetiologic factors and leads to tear film instability, ocular surface damage and neurosensory changes. Symptoms of DED include ocular dryness, burning, itching, pain and visual impairment. An evidence-based global consensus on multiple aspects of DED is proposed by the Tear Film & Ocular Surface Society (TFOS) Dry Eye Workshop (DEWS) III.
The 2025 TFOS DEWS III report updates the recommendations and conclusions of the 2017 TFOS DEWS II regarding the subclassification, screening and diagnostic methodology, and management and therapy of DED [1-4]. It provides a timely overview of current evidence on the management of patients with DED, emphasising the need to tailor treatment to specific diagnostic and aetiologic factors for more targeted and effective management.
Diagnostic methodology
The TFOS DEWS III acknowledges that DED is a multifactorial disease that is always symptomatic. A revised definition underscores that the homeostasis of the ocular surface environment and that of the tear film has the potential to be disrupted in DED: “Dry eye is a multifactorial, symptomatic disease characterised by a loss of homeostasis of the tear film and/or ocular surface, in which tear film instability and hyperosmolarity, ocular surface inflammation and damage and neurosensory abnormalities are aetiological factors” [1,2].
Dry eye disease remains a specific symptomatic subset of ocular surface disease and differential diagnosis is important to rule out conditions that can mimic DED [1]. DEWS III provides guidance on differential diagnosis and ocular examination, together with the risk factors that should be discussed with the patient.
Available evidence demonstrated that the screening questionnaires recommended in 2017 do not offer comparable measures of symptoms. In order to standardise diagnosis in clinical practice, DEWS III recommends use of a single questionnaire for symptom screening. The recommended screening questionnaire is the OSDI-6, the shortened form of the Oxford Surface Disease Index (OSDI), with a cut-off score ≥4. OSDI-6 results can be indexed against severity, as normal (0–3 points), mild-to-moderate DED (4–8 points) or severe DED (>8 points) [2].
The 2017 DEWS II report emphasised that DED encompasses a broader mix of subtypes and different aetiologies than that captured by current classification methods, typically characterised by two main DED subgroups, namely ‘evaporative’ and ‘aqueous-deficient’ dry eye. The former subtypes of aqueous deficient and evaporative DED have been replaced with a revised subclassification, separated into:
- Tear film deficiencies (lipid, aqueous and mucin/glycocalyx)
- Eyelid anomalies (blink/lid closure and lid margin), and
- Ocular surface abnormalities (anatomical misalignment, neural dysfunction, ocular surface cell damage/disruption and primary inflammation/oxidative stress).
Appropriate clinical tests and cut-offs have been provided to identify these aetiological drivers in an individual, and in turn inform appropriate management and therapy [1]. Figure 1 summarises recommendations for diagnosis and subtyping of DED [2].
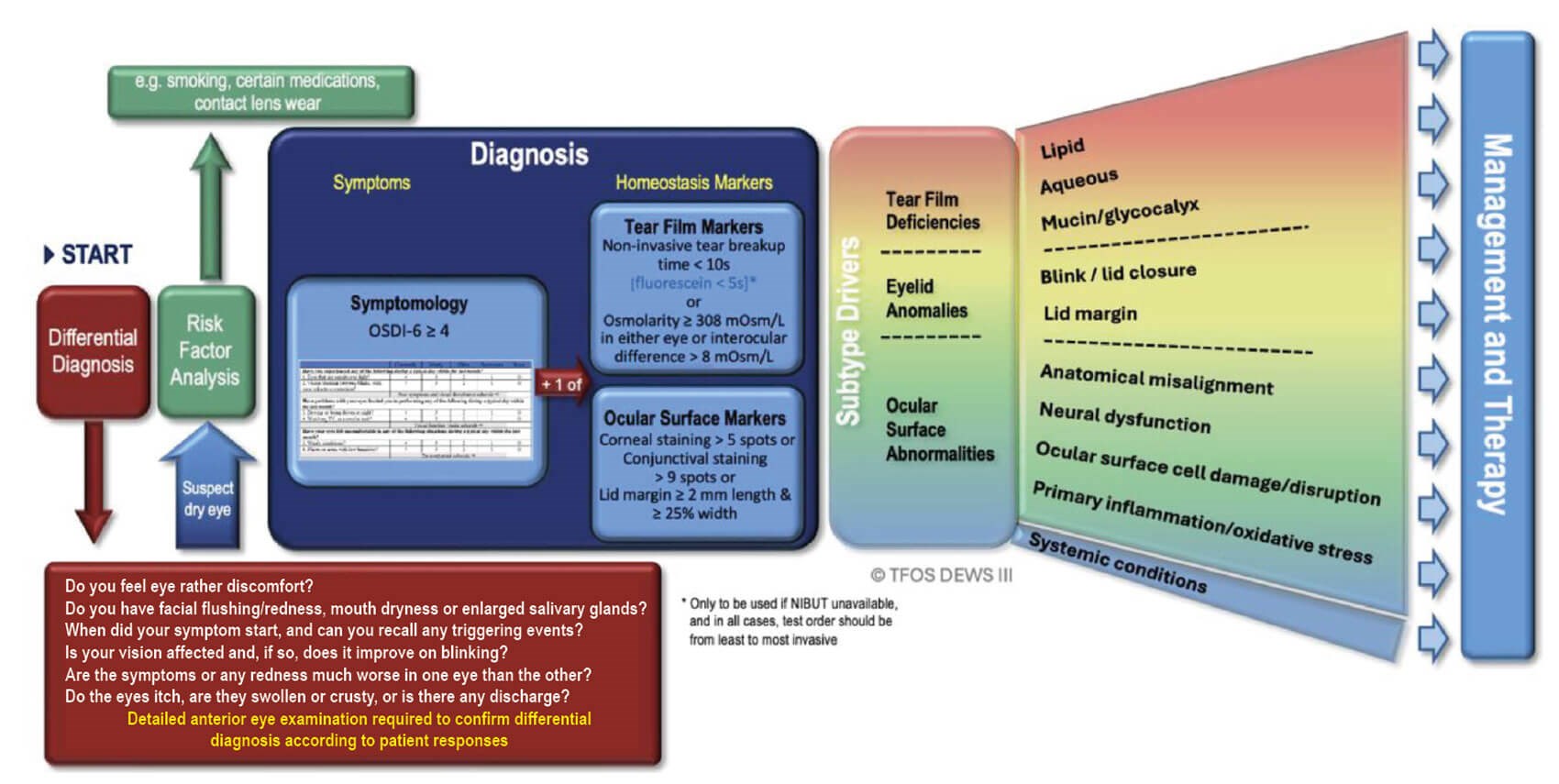
Figure 1: Diagnosis and subtyping of DED to inform restoration of tear film and ocular surface homeostasis through appropriate management and therapy. Source: Perez VL, Chen W, Craig JP, et al. TFOS DEWS III: Executive Summary. Am J Ophthalmol 2026;282:125–45. Creative Commons CC-BY-4.0 license.
A confirmed diagnosis of DED is based on an OSDI-6 score ≥4 combined with one or more of the following signs of loss of homeostasis:
- Tear film markers:
- A non-invasive breakup time <10s or tear film hyperosmolarity (≥308 mOsm/L in either eye or an interocular difference >8 mOsm/L) - Ocular surface staining:
- Corneal fluorescein staining of >5 punctate spots, and/or
- Lissamine green conjunctiva staining >9 punctate spots, and/or
- Lissamine green lid margin staining of ≥2mm length and ≥25% width.
In a patient with a positive OSDI-6 screening of dry eye symptoms but with no ocular surface staining, only non-invasive tear breakup time or osmolarity needs to be measured to confirm the presence or absence of DED.
Management and therapy
The TFOS DEWS III report on management and therapy provides evidence-based algorithms to support clinicians in the management of patients with DED [3]. The authors note that a number of listed treatments overlap with other broad areas of management due to overlapping mechanisms of action. The report highlights evidence to support or inform the use of the listed management options to treat one or more of the updated subclassifications of DED.
Lifestyle advice
Lifestyle factors contribute to both the development and management of DED. Excessive digital device use is considered one of the most significant contributors to DED and patients should reduce screen time or take regular breaks to improve blink rate. Specific lifestyle considerations for all individuals with DED, regardless of subtype and the management options proposed, include (a) avoidance of factors that precipitate symptoms of DED, (b) control of the local environment and (c) physical protection. Nocturnal lagophthalmos may worsen DED. Omega-3 fatty acids show modest benefit and hydration is essential. Lifestyle advice includes avoid smoking and allergens and to manage systemic conditions like Sjögren’s syndrome.
Tear insufficiency and meibomian gland dysfunction (MGD)
The cornerstone of DED treatment remains tear supplementation and stabilisation of the tear film [1,3]. The goal of these therapies is to restore homeostasis of the tear film and ocular surface microenvironment, in many cases by stabilising the preocular tear film. The authors note the move towards using preservative-free unit-dose formulations, less damaging preservatives such as stabilised oxychloro complex or sodium perborate, or the use of multi-dose, preservative-free bottles specifically designed to prevent contamination with microorganisms.
The report states that clinical studies have demonstrated tear supplements containing polymer combinations outperform single-polymer formulations in terms of DED symptom relief, tear film stability and patient satisfaction [3]. Available evidence suggests that patients with lipid deficiency benefit most from lipid containing supplements. In a randomised controlled trial, Craig, et al. observed that, over a six-month treatment period, improvements in dry eye symptomology preceded tear film and ocular surface changes with regular use of both lipid and non-lipid-based artificial tear supplements. Both formulations addressed most mild-to-moderate forms of aqueous deficient and evaporative DED, while the latter benefitted preferentially from lipid-based supplementation [5].
A one-month treatment trial of regular daily use is likely to help determine whether a particular artificial tear supplement will be effective for symptom relief. An extended treatment trial of two to four months may be required to observe an effect on signs of DED [2].
Tear conservation
TFOS DEWS III reviewed contact lenses, moisture-retaining spectacles and punctal plugging. Scleral contact lenses provide the therapeutic benefit of both enhancing visual function and improving the ocular surface health and it is essential to ensure optimal fitting. The report comments that scleral lens use is generally not linked to significant complications (noting the common challenge of midday fogging) and effectively improves the symptoms and signs of DED.
Tear stimulation
TFOS DEWS II suggested that intense pulsed light (IPL) therapy was an effective and safe approach to treat MGD and DED. Since its publication, a number of clinical trials have evaluated IPL, largely as a treatment for moderate to advanced MGD, demonstrating reduction in symptoms and signs of DED, improved optical quality, supporting an improved tear film lipid layer, and reduced dependence on tear supplementation. The degree of efficacy and its duration varied depending on concomitant treatment and number of treatment sessions. Unlike IPL, low-level light therapy (LLLT) can be applied directly to the eyelids and, according to DEWS III, it is often considered most effective when combined with other treatments for DED.
Device-driven and pharmacological neuromodulation are both reviewed. Options for pharmacological neuromodulation include acoltremon (TRYPTYR, Alcon), a potent and highly selective transient receptor potential melastatin 8 (TRPM8) agonist and varenicline intranasal spray (Tyrvaya, Oyster Point Pharma, Inc.).
In July 2025, Alcon announced the US launch of TRYPTYR (acoltremon ophthalmic solution) 0.003% as a new prescription treatment option for dry eye [6]. TRYPTYR is a TRPM8 thermoreceptor agonist indicated for the treatment of the signs and symptoms of DED. In two (COMET-2 and COMET-3) randomised, double-masked, vehicle controlled multisite clinical studies in subjects with dry eyes, TRYPTYR 0.003% demonstrated a statistically significant improvement in tear production. The most common ocular adverse reaction observed in controlled clinical studies was instillation site pain (50%). Less than 1% of patients discontinued therapy due to burning or stinging sensation in the eyes.
Treatments for eyelid abnormalities include management and therapy of blink and lid closure anomalies, along with methods to reduce eyelid microbial load and manage MGD.
Anti-inflammatory pharmacological therapies
Topical anti-inflammatory pharmacological therapies for DED include corticosteroids and T-cell immunomodulatory topical drugs. A Cochrane systematic review published in 2022 concluded that, for dry eye patients whose symptoms require anti-inflammatory control, topical corticosteroids probably provide small-to-moderate degrees of symptom relief beyond lubricants and may provide small-to-moderate degrees of symptom relief beyond cyclosporine A (CsA). Current evidence is considered less certain about the effects of steroids on improved tear film quality or quantity [7]. DEWS III notes that subtyping of the DED present is an important factor for appropriate patient selection when considering prescribing topical steroids.
Surgical treatments
DEWS III highlights surgical interventions for ocular surface abnormalities that affect anatomical alignment of the lid and globe and management of lid anomalies; these include permanent punctal occlusion, tarsorrhaphy, surgical management of lid abnormalities (botulinum toxin injection, dermatochalasis, entropion and ectropion), surgical management of anatomical surface abnormalities (conjunctivochalasis, pterygium and pinguecula), salivary gland transplantation and reinnervation of the lacrimal gland.
Prescribing algorithm
TFOS DEWS III acknowledges that simple division of patients into broad subgroups of aqueous deficient or evaporative dry eye fails to recognise that multiple drivers of signs and symptoms exist that may be present simultaneously, which may vary over time and with treatment compliance. The TFOS DEWS III diagnostic methodology report provides guidance to help clinicians identify the most likely clinically relevant drivers of a patient’s dry eye [2].
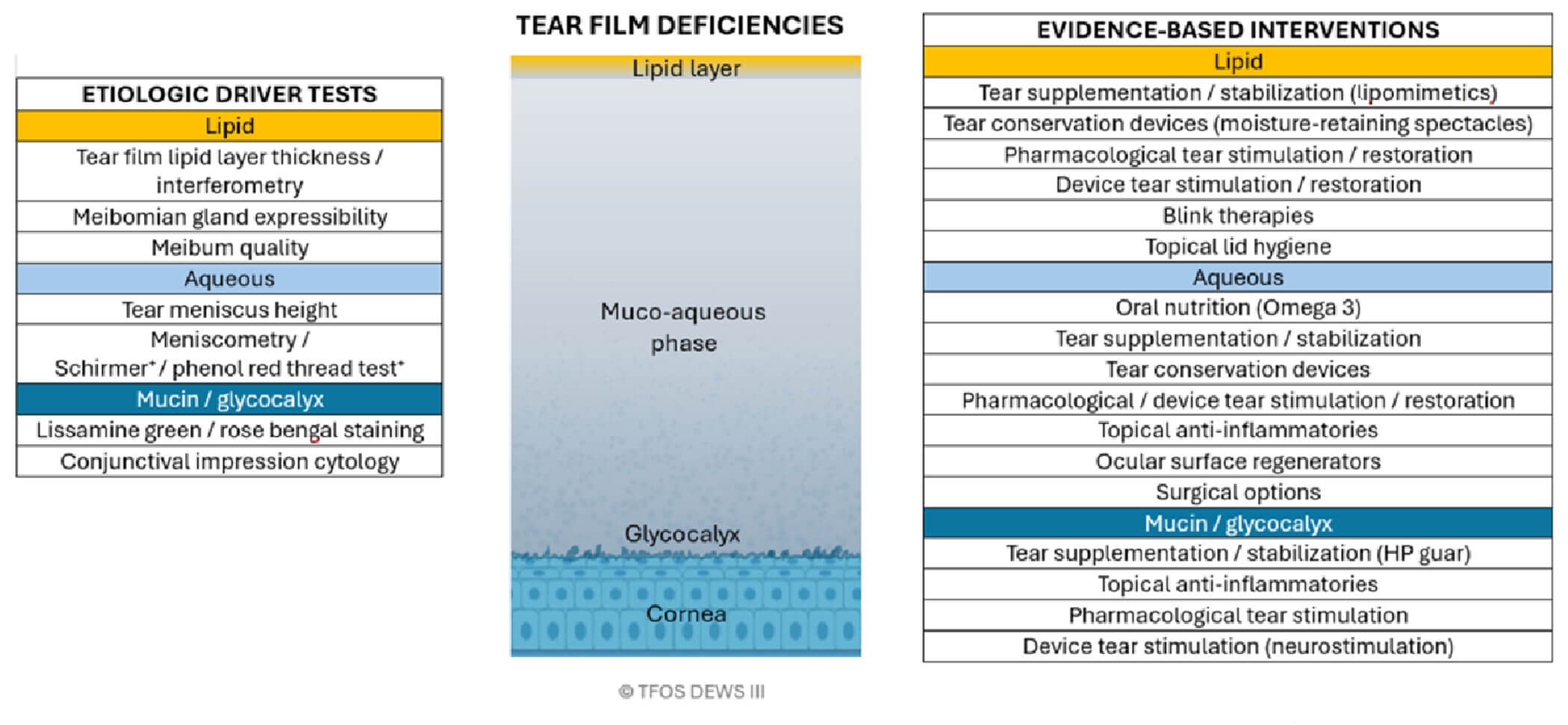
Figure 2: Diagnostic tests and evidence-based interventions to manage the aetiologic drivers associated with tear film deficiency-related subtypes of DED. Source: Perez VL, Chen W, Craig JP, et al. TFOS DEWS III: Executive Summary. Am J Ophthalmol 2026;282:125–45. Creative Commons CC-BY-4.0 license.
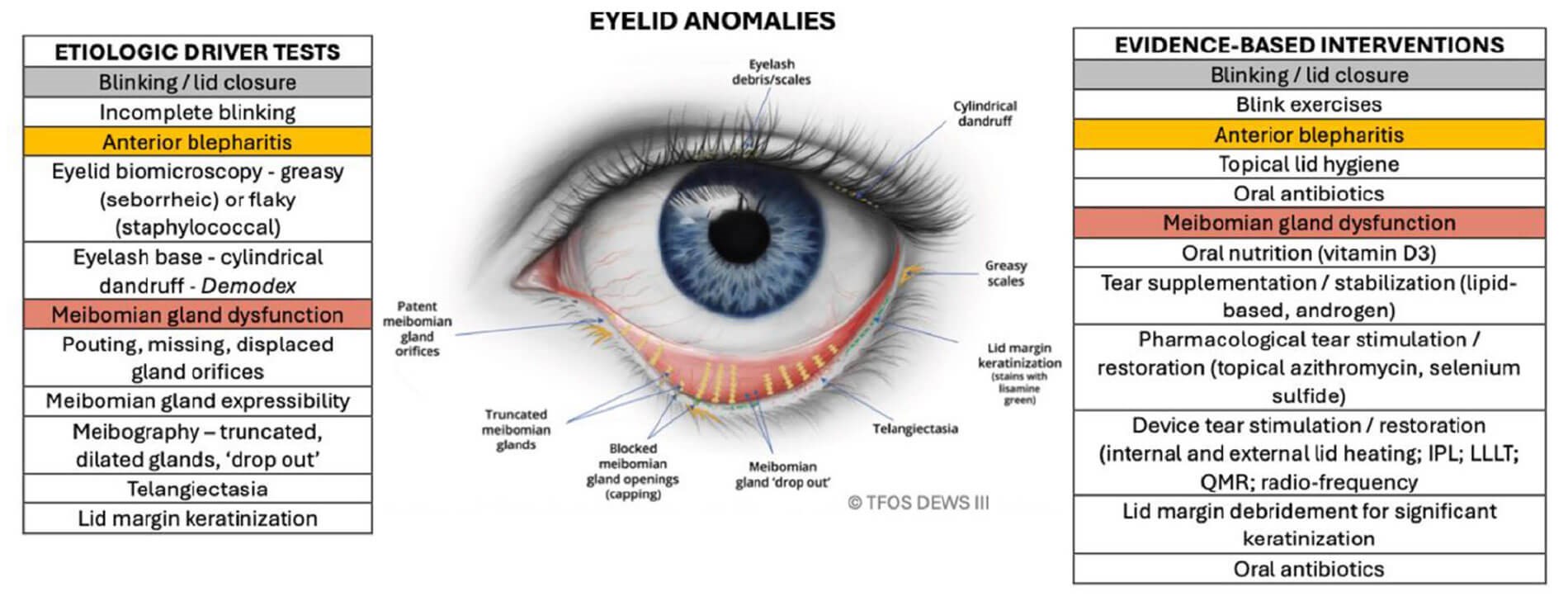
Figure 3: Diagnostic tests and evidence-based interventions to manage the aetiologic drivers associated with eyelid-related subtypes of DED. Source: Perez VL, Chen W, Craig JP, et al. TFOS DEWS III: Executive Summary. Am J Ophthalmol 2026;282:125–45. Creative Commons CC-BY-4.0 license.
Evidence-based treatment approaches are linked to the three aetiological subtypes, categorised as tear component deficiencies (Figure 2), eyelid anomalies (Figure 3) and ocular surface abnormalities (Figure 4) [1,3]. DEWS III emphasises that multiple treatments in combination are often required to address the multiple pathogenic drivers of DED. Moreover, sustained clinical improvement often necessitates comprehensive patient education on lifestyle factors and adherence to the prescribed management plan.
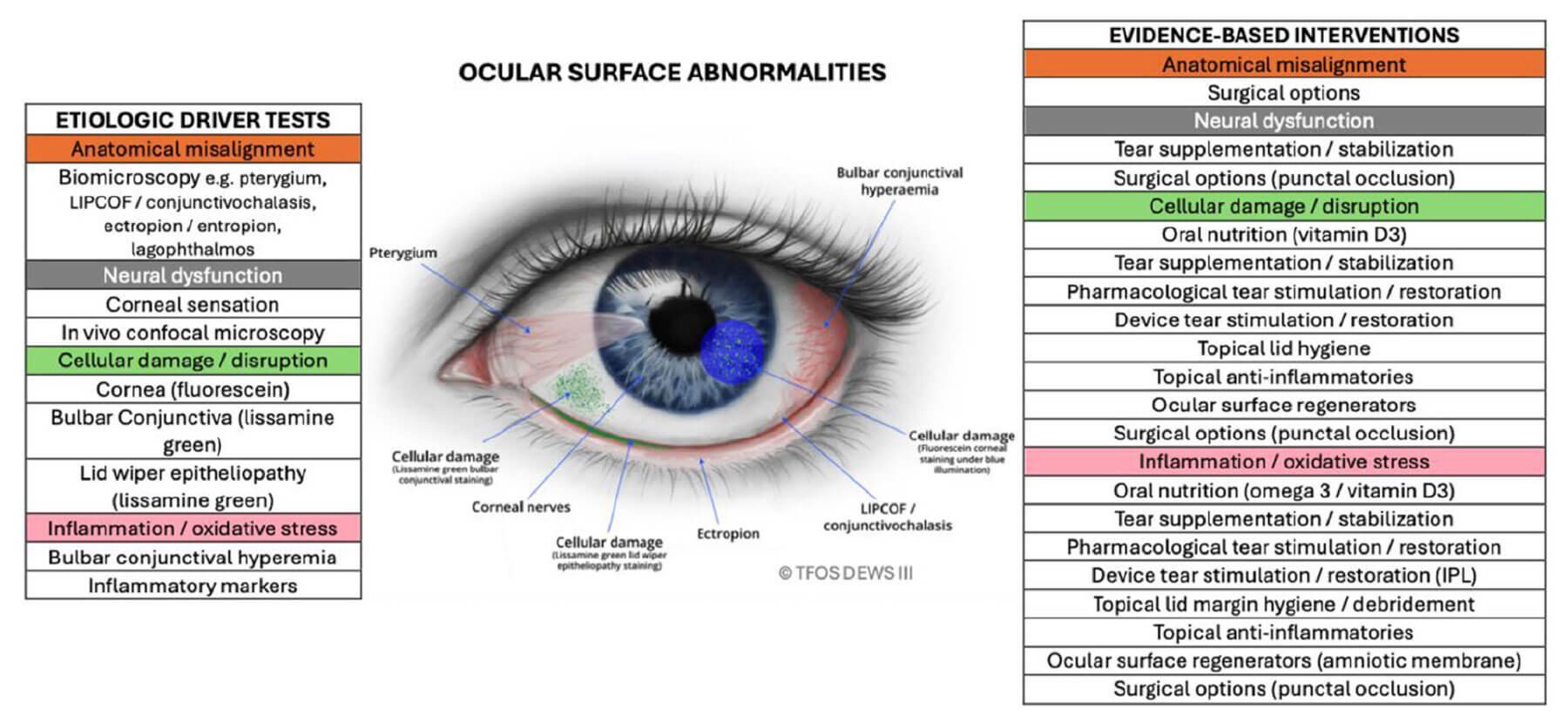
Figure 4: Diagnostic tests and evidence-based interventions to manage the aetiologic drivers associated with ocular surface-related subtypes of DED. Source: Perez VL, Chen W, Craig JP, et al. TFOS DEWS III: Executive Summary. Am J Ophthalmol 2026;282:125–45. Creative Commons CC-BY-4.0 license.
In summary
- Ocular lifestyle modifications, tear film supplements and environmental adjustments to stabilise the tear film are recommended as first line management.
- Meibomian gland dysfunction, a major contributor to evaporative DED, is addressed through warm compresses, lid massage, in-office heating devices, IPL, LLLT and emerging topical drugs.
- Anti-inflammatory therapies such as corticosteroids, CsA and lifitigrast, along with biologic tear substitutes, may be considered for patients with primary inflammatory or immune-mediated components.
- Novel pharmaceutical and neuromodulatory therapies have shown promise for enhancing tear production.
- Amniotic membrane grafts and various advanced surgical options are available for refractory or severe DED cases.
Practitioner viewpoint
Ernesto J Otero, Professor of Ophthalmology, Barraquer Institute of America, presented at the cornea subspecialty day during the American Academy of Ophthalmology 2025 annual meeting on an evidence-based approach to interventions for dry eye [8]. He noted that there are a multitude of different treatment options for dry eye, together with an overwhelming number of related publications. He stressed that the goal of physicians is to assess which evidence is relevant and significant. He suggested a phased treatment approach based on underlying aetiology and severity of DED.
A systematic review published in 2019 concluded that long-chain omega-3 supplements may have little or no benefit, relative to placebo, on dry eye symptoms, but did improve some clinical signs [9]. It noted that there was a beneficial effect on dry eye symptoms when omega-3 supplements were combined with standard dry eye treatments (e.g. artificial tears, eyelid warm compresses, corticosteroid eye drops) compared to standard treatment alone and when long-chain omega-3 supplements were compared with omega-6 supplements.
A meta-analysis review of punctal occlusion for dry eye syndrome published in 2017 noted that evidence suggests that punctal plugs do not conclusively improve dry eye symptoms and it is still unclear if punctal plugs are better than oral treatment (oral pilocarpine) or eye drops such as cyclosporine or artificial tears [10].
A Cochrane review from 2020 evaluated IPL therapy for the treatment of MGD, concluding that, due to limited information in the clinical trials reviewed, it was not possible to determine with certainty whether IPL treatment for MGD is effective or safe [11]. They noted that IPL therapy may be helpful to improve some of the clinical signs of MGD, such as tear stability and tear composition, but were unclear about the effect of IPL on meibomian gland blockage or corneal sodium fluorescein staining.
Given the preponderance of low-certainty evidence, what can clinicians rely upon? The TFOS DEWS III is a worldwide initiative to review and analyse evidence relating to dry eye, explained Prof Otero. The main aims were to provide an evidence base review of the management and therapy of patients with DED (treatment options divided into 10 sub-categories) and provide an algorithm to assist clinicians on treatment options and their use based on signs and symptoms.
In summarising key takeaways from TFOS DEWS III, Prof Otero noted that an evidence-based approach to dry eye patients translates relevant robust research evidence into clinical practice. The TFOS DEWS Ill provides an evidence-based framework for the management and therapy of patients with dry eye disease and proposes several treatment algorithms to assist clinicians on when to use these therapies based on signs and symptoms. He concluded by underscoring the need for more robust randomised control trial and level II evidence to enhance practitioners’ knowledge and understanding of therapies for DED.
References
1. Perez VL, Chen W, Craig JP, et al. TFOS DEWS III: Executive Summary. Am J Ophthalmol 2025;282:134–45.
2. Wolffsohn JS, Benítez-Del-Castillo JM, Loya-Garcia D, et al. TFOS DEWS III: Diagnostic Methodology. Am J Ophthalmol 2025;279:387–450.
3. Jones L, Craig JP, Markoulli M, et al. TFOS DEWS III: Management and Therapy. Am J Ophthalmol 2025;279:289–386.
4. Stapleton F, Argüeso P, Asbell P, et al. TFOS DEWS III: Digest. Am J Ophthalmol 2025;279:451–553.
5. Craig JP, Muntz A, Wang MTM, et al. Developing evidence-based guidance for the treatment of dry eye disease with artificial tear supplements: A six-month multicentre, double-masked randomised controlled trial. Ocul Surf 2021;20:62–9.
6. https://www.accessdata.fda.gov/
drugsatfda_docs/label/2025/
217370s000lbl.pdf
[Link last accessed December 2025]
7. Liu SH, Saldanha IJ, Abraham AG, et al. Topical corticosteroids for dry eye. Cochrane Database Syst Rev 2022;10(10):CD015070.
8. Otero EJ. Interventional dry eyes: an evidence-based approach. Presentation at American Academy of Ophthalmology annual meeting Cornea subspecialty day 2025.
9. Downie LE, Ng SM, Lindsley KB, Akpek EK. Omega-3 and omega-6 polyunsaturated fatty acids for dry eye disease. Cochrane Database Syst Rev 2019;12(12):CD011016.
10. Ervin AM, Law A, Pucker AD. Punctal occlusion for dry eye syndrome. Cochrane Database Syst Rev 2017;6(6):CD006775.
11. Cote S, Zhang AC, Ahmadzai V, et al. Intense pulsed light (IPL) therapy for the treatment of meibomian gland dysfunction. Cochrane Database Syst Rev 2020;3(3):CD013559.
Declaration of competing interests: The author has provided consultancy services to Bayer AG, DORC International B.V., Johnson & Johnson Vision Care, Inc., Roche Products Ltd and Thea Pharmaceuticals Ltd.





