Stevens–Johnson syndrome (SJS) is an uncommon dermatological emergency on the same clinical spectrum as toxic epidermal necrolysis (TEN). SJS is characterised by an acute, immune-mediated attack on the skin and mucous membranes, producing a rapidly progressive erythematous eruption with blistering and epithelial sloughing affecting <10% of body surface area, whereas TEN involves more extensive epithelial detachment and carries higher mortality.
Most cases arise from a delayed type IV hypersensitivity reaction to medication metabolites, typically within the first few weeks of exposure or dose change. Less commonly, infections such as mycoplasma pneumoniae are implicated via mechanisms such as molecular mimicry.
Ocular involvement is frequent (roughly half to four fifths of patients) and may span the acute phase – conjunctival hyperaemia, membranous conjunctivitis and corneal epithelial defects – to chronic sequelae including symblepharon, lid margin keratinisation, limbal stem cell deficiency, scarring and sight-threatening corneal complications. Early ophthalmic assessment and prompt surface protective treatment are therefore critical to reduce irreversible damage and preserve vision [1-3].
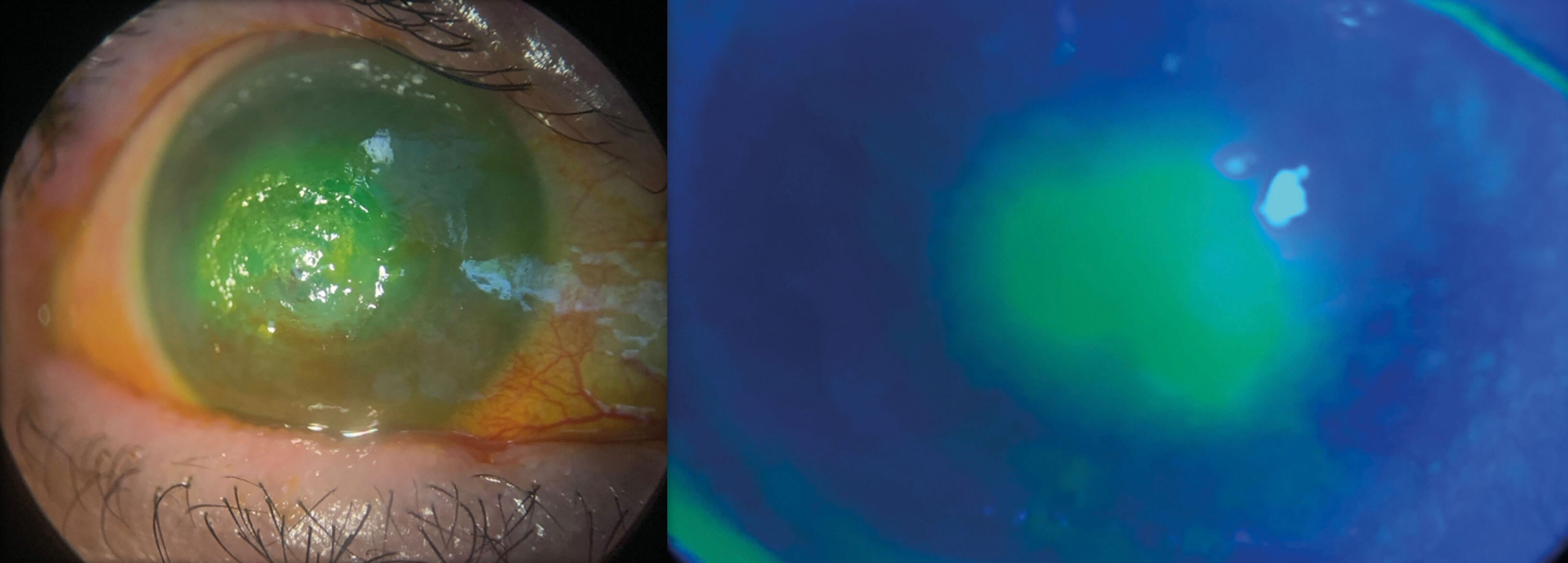
Figure 1: Persistent epithelial defect following AMG.
We present a case of severe ocular SJS presumed secondary to trimethoprim exposure, illustrating the iterative medical and surgical strategies required to maintain the ocular surface in the face of recurrent epithelial breakdown, infection and perforation.
Case report
A 60-year-old woman presented with a prodrome of fever, malaise and cough followed by a rapidly spreading mucocutaneous eruption and oral/urogenital ulcers. Two weeks earlier she had been treated for a urinary tract infection with trimethoprim. On arrival, she reported severe odynophagia, dysuria, striking photosensitivity and reduced vision. She was tachycardic, hypotensive and febrile. She was admitted directly to intensive care for resuscitative management.
Dermatology confirmed SJS on clinical grounds and punch biopsy demonstrating keratinocyte necrolysis. Ophthalmology reviewed the patient after haemodynamic stabilisation. Visual acuity was reduced to counting fingers in both eyes. There was lid margin ulceration, confluent conjunctival epithelial loss and corneal defects bilaterally. The ocular surface was immediately protected with bilateral amniotic membrane grafts (AMG) and fornix conformers to prevent early forniceal shortening. Topical therapy comprised hourly preservative-free lubricants, moxifloxacin 0.5% six times daily and preservative free dexamethasone 0.1%.
At one week, the conformers had dissolved and large, persistent epithelial defects remained. Amniotic membrane discs with bandage contact lenses (BCLs) were applied. Multiple misdirected lashes were noted and epilated. Autologous serum eye drops were initiated, yet progressive corneal thinning was observed, culminating in a corneal perforation in the right eye. Urgent repeat AMG with temporary tarsorrhaphy was performed.
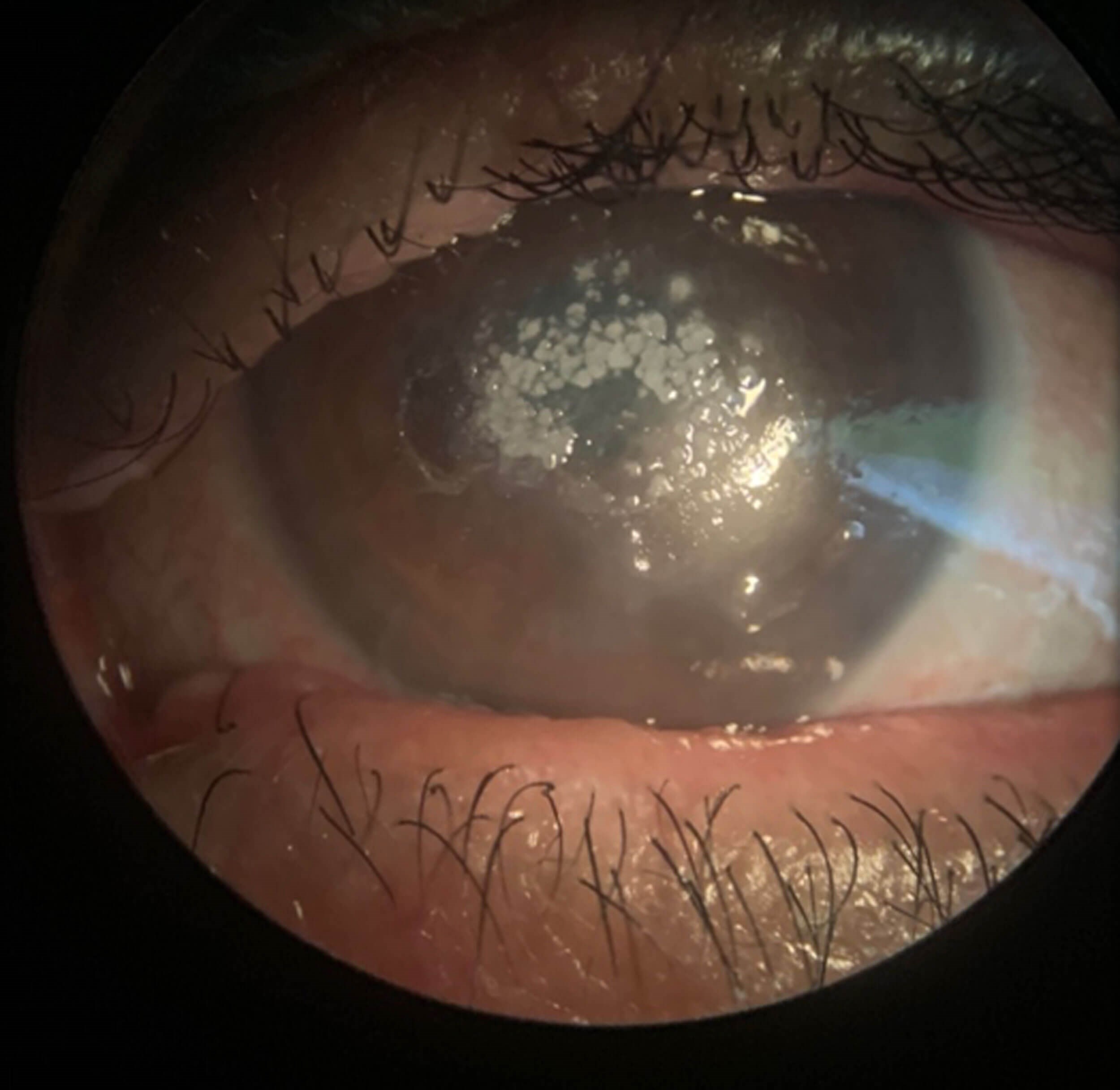
Figure 2: Candida keratitis.
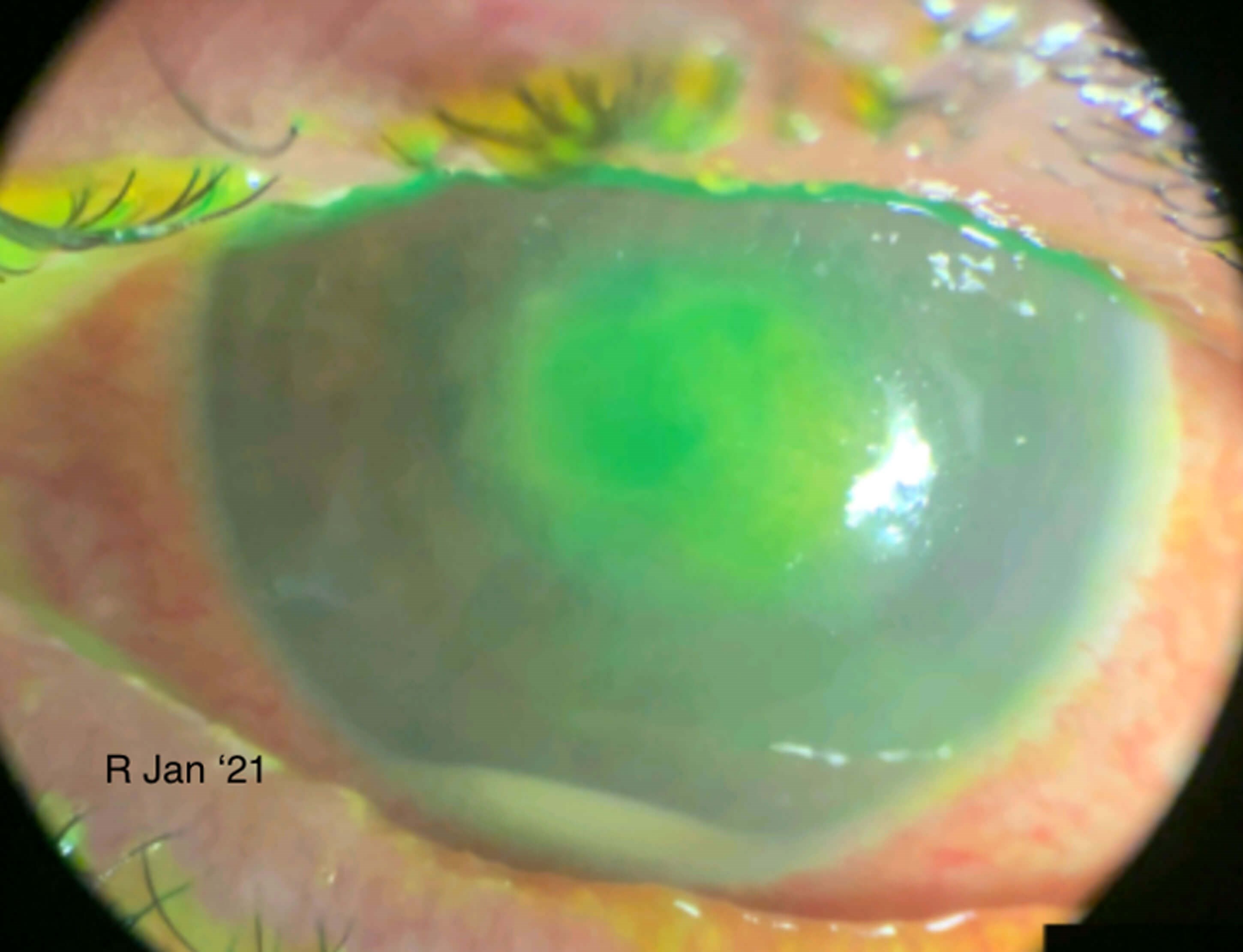
Figure 3: Sterile hypopyon secondary to worsening inflammation.
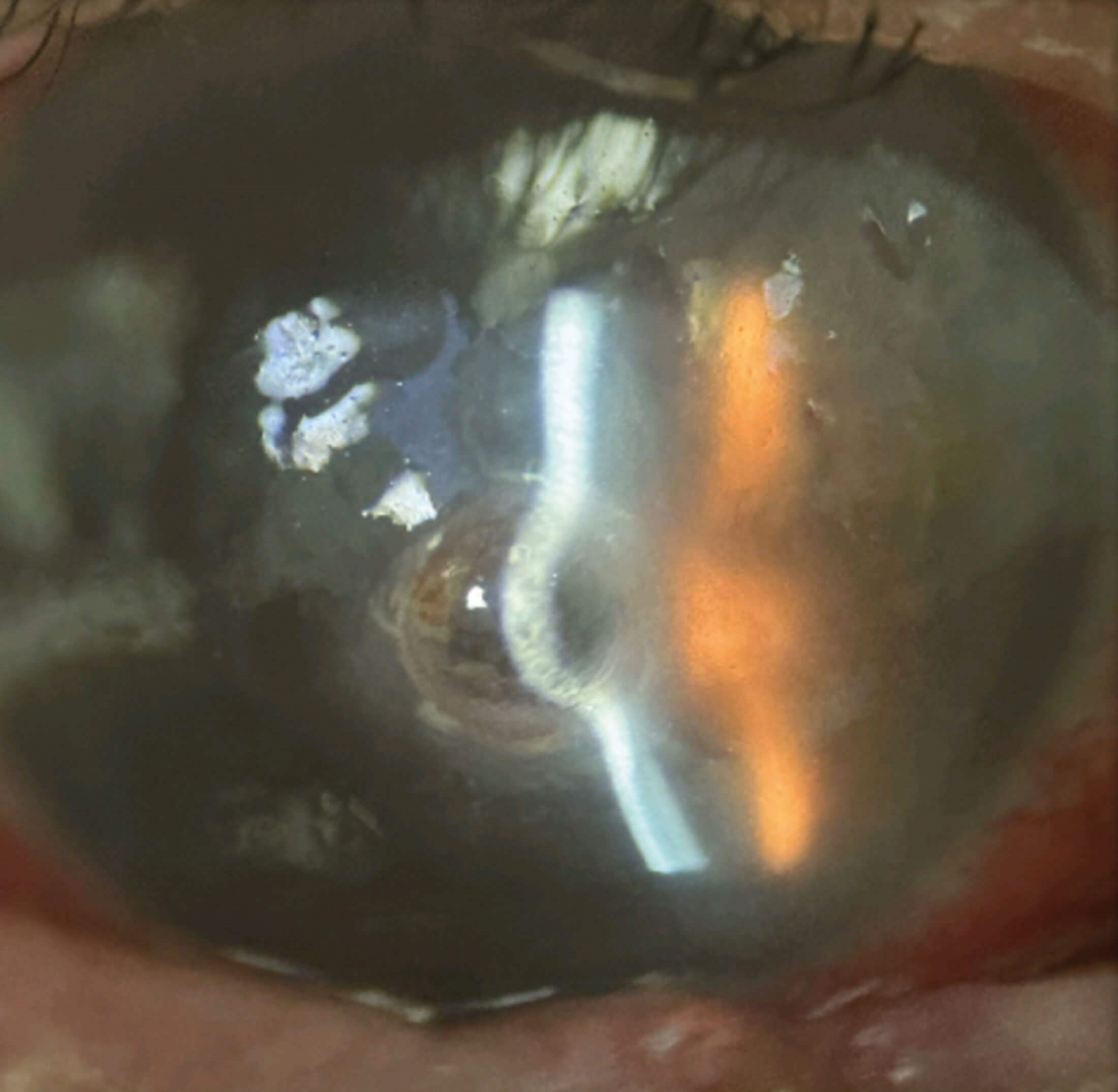
Figure 4: Left eye descemetocele.
Initial postoperative review showed transient improvement, and the drop regimen of antibiotics, topical steroids, intensive lubricants and serum drops was continued. Two weeks later, the right eye developed a recurrent leak requiring cyanoacrylate glue and BCL. Recurrent trichiasis necessitated frequent epilation.
Subsequently the patient re-presented acutely with bilateral pain and injection. Corneal scrapes and polymerase chain reaction (PCR) testing grew Candida, consistent with fungal keratitis. Topical voriconazole was commenced and corticosteroids were withheld; intraocular inflammation worsened transiently with a sterile hypopyon before settling as the infiltrates responded. Botox-induced temporary ptosis was used adjunctively to protect the surface and reduce exposure- related trauma. A further small perforation ensued and was again treated with tissue adhesive.
Over the following weeks, the left eye deteriorated with formation of a descemetocele. Given the severe aqueous deficiency and exposure risk, permanent punctal occlusion by thermal cautery was performed bilaterally to conserve tears and stabilise the surface. Despite intensive therapy, the patient’s vision remained at hand movements in both eyes across most visits. The left eye evolved to dense corneal vascularisation with lipid keratopathy, while the right eye continued to suffer recurrent epithelial breakdown.
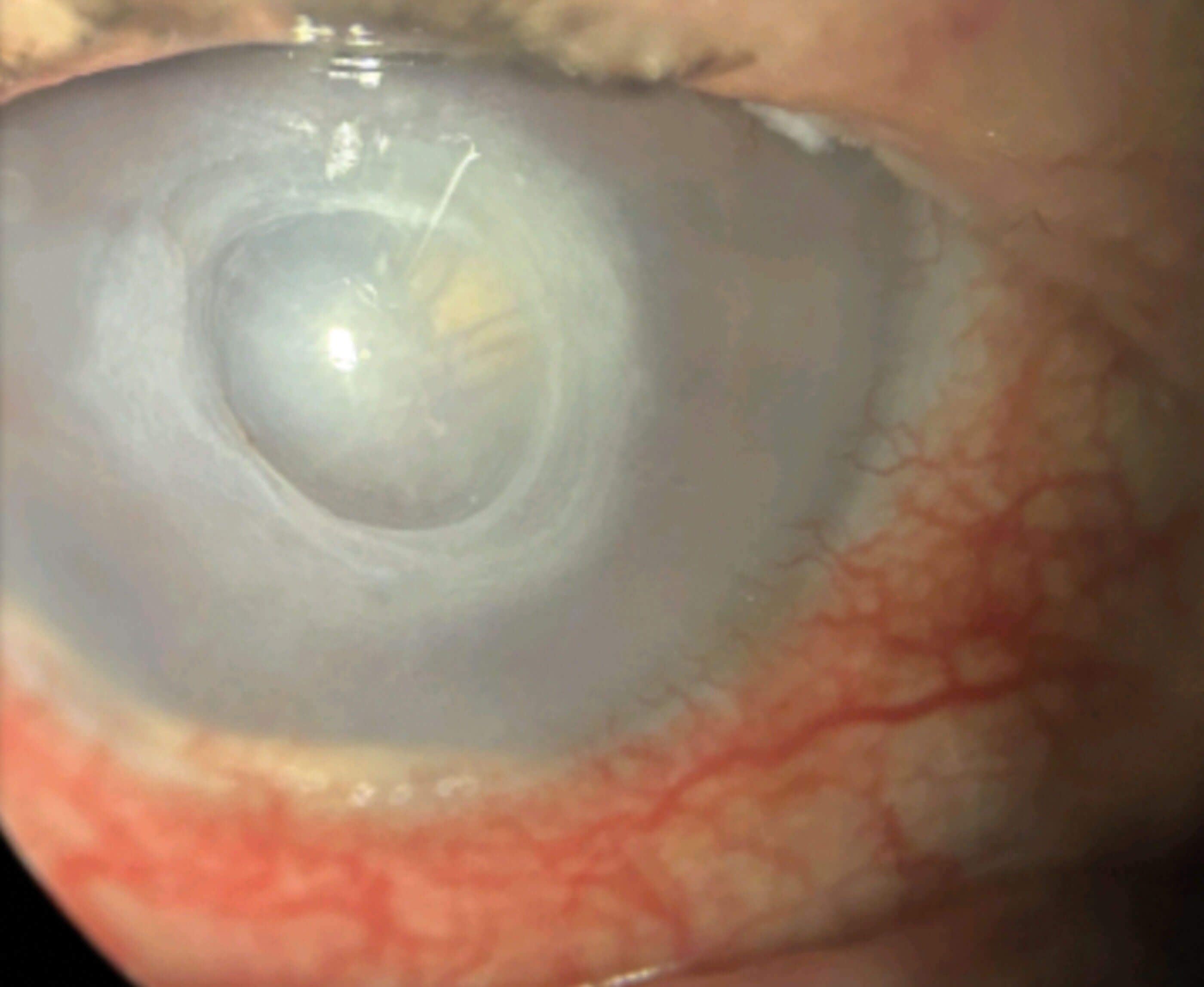
Figure 5: Right eye persistent epithelial defect prior to penetrating keratoplasty (PK).
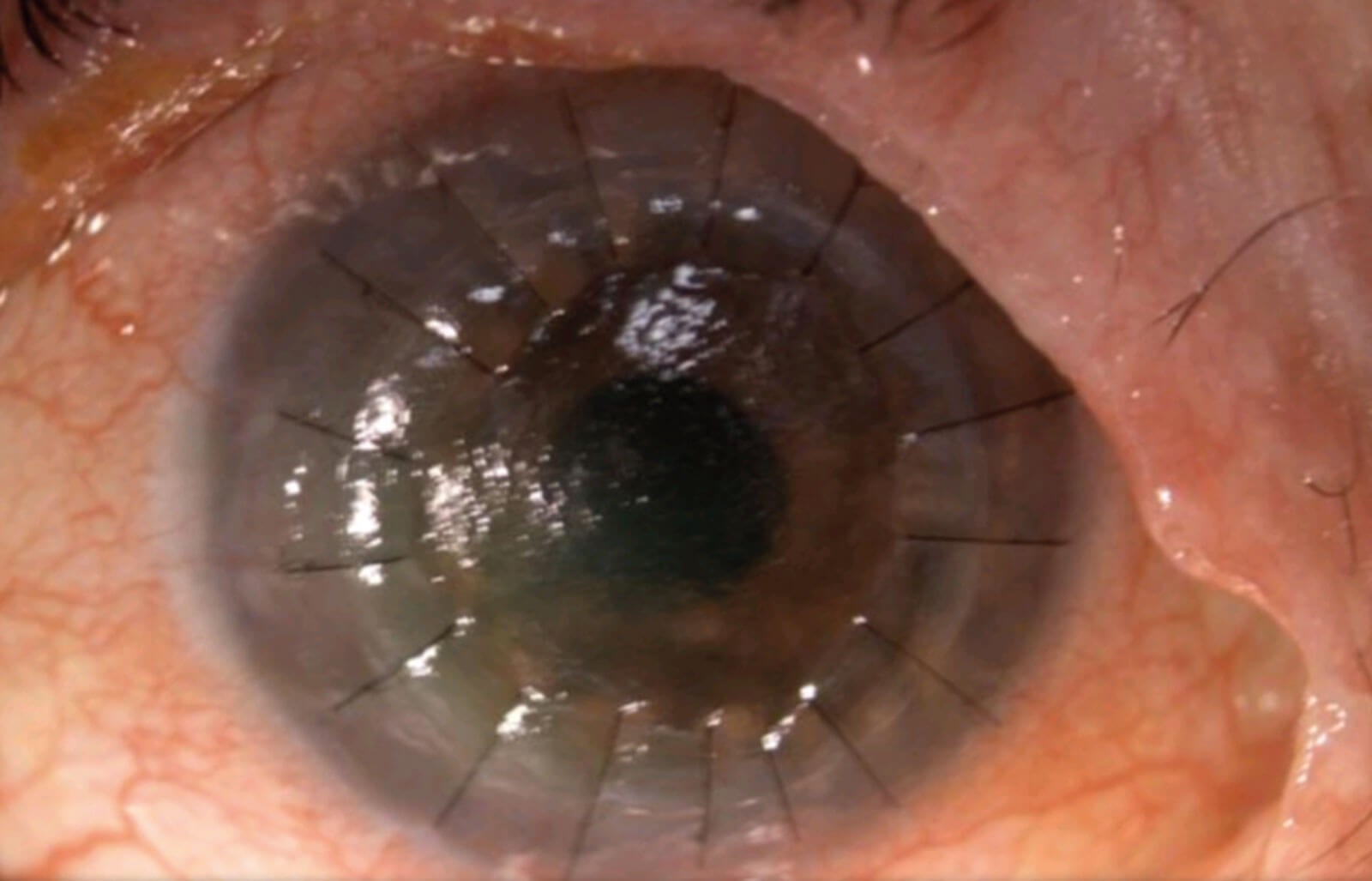
Figure 6: Right eye epithelial defect following PK.
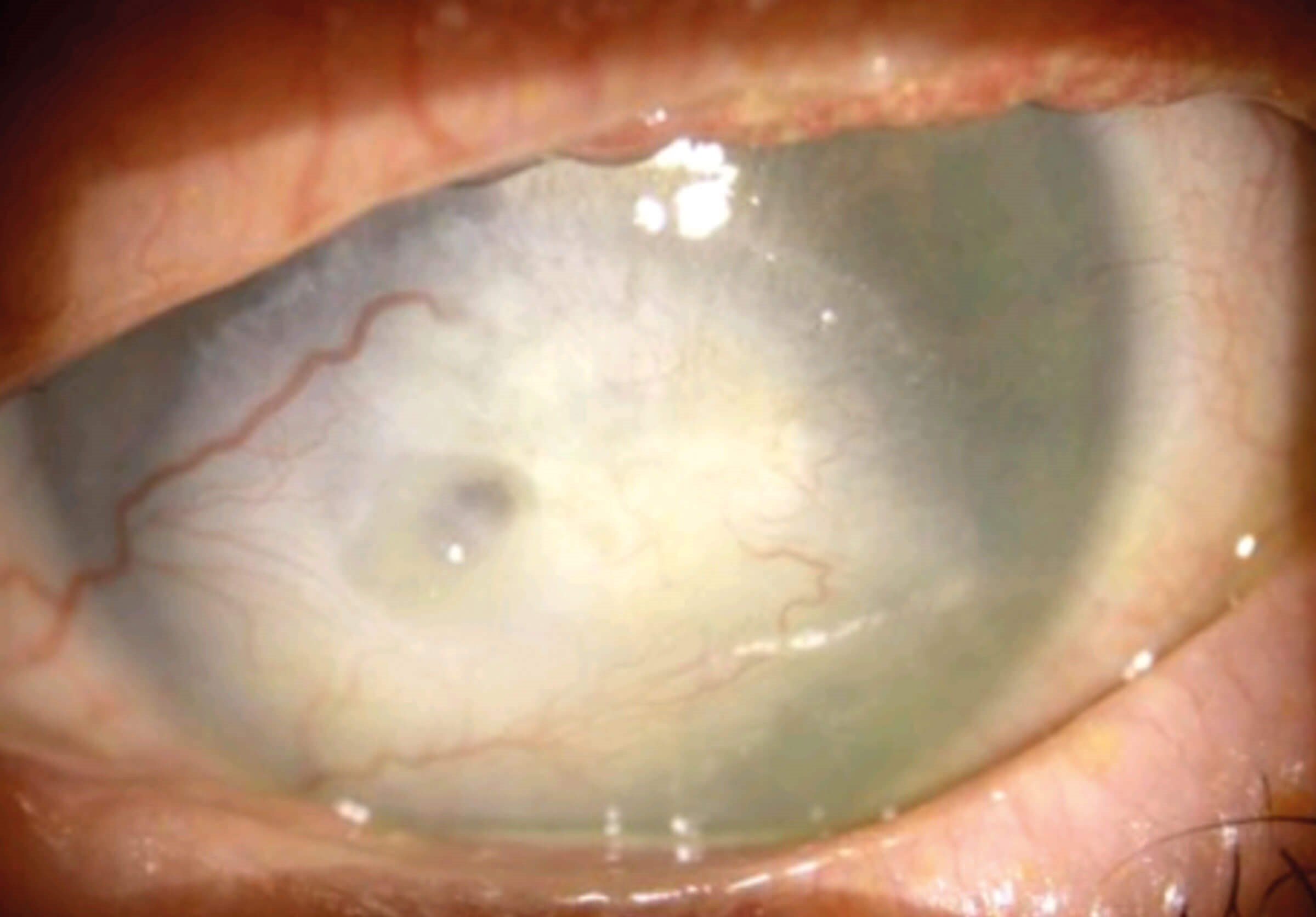
Figure 7: Current finding in left eye.
With the ocular surface sufficiently quietened, a tectonic penetrating keratoplasty (PK) was performed in the right eye. Early graft reviews showed persistent epithelial defects on the transplant, managed with enhanced lubrication, BCL and optimisation of lid hygiene and lash control. The left eye retained a vascularised, scarred cornea with reduced comfort but no further perforation at the latest review.
Discussion
This case exemplifies the chronic, relapsing nature of ocular surface disease in SJS and the need for early, protocol driven, multidisciplinary care. Ocular involvement in SJS/TEN is common and ranges from mild conjunctivitis to severe cicatrising keratoconjunctivitis with blinding sequelae. Evidence-based acute management focuses on rapid epithelial rescue, infection control and inflammation modulation while protecting adnexal anatomy [2,3]. Topical preservative free lubricants, prophylactic antibiotics for epithelial defects, and cautious topical corticosteroids for acute inflammation are standard; adjunctive immunomodulators (e.g. topical ciclosporin) and scleral lenses can support surface rehabilitation in selected patients [3]. Systemic therapy – corticosteroids, cyclosporine, intravenous immunoglobulin – may be considered in the broader management of SJS/TEN and may help limit ocular surface damage in some series [1,2].
Amniotic membrane transplantation (AMT) is widely advocated in the acute phase for its anti-inflammatory, anti- fibrotic and epithelialising properties. Early placement – often within 5–10 days of symptom onset – reduces the risk of late scarring, symblepharon, limbal stem cell deficiency and lid-related sequelae, and the membrane typically dissolves within 3–14 days [3,4]. Our patient received timely AMG yet still progressed to epithelial failure and perforation, emphasising that even optimal early therapy cannot always avert severe outcomes, particularly when compounded by adnexal disease (trichiasis, lid margin ulceration) and tear film failure.
The eyelids and tear drainage system are central to long-term ocular surface stability after SJS. Lid margin keratinisation is a major driver of mechanical microtrauma; strategies such as epilation of trichiatic lashes, Botox-induced ptosis, temporary or permanent tarsorrhaphy, anterior lamellar repositioning and lateral canthoplasty protect the cornea from blink related injury [3–5]. In refractory aqueous deficiency, punctal occlusion – via plugs or cautery – is an effective measure to conserve tears and improve epithelial health. We used permanent cautery given the severity and persistence of surface breakdown.
Superinfection is a recognised complication in the setting of epithelial defects, topical steroids and contact lenses. Our patient’s candida keratitis necessitated prompt antifungal therapy and steroid withdrawal, which, while microbiologically appropriate, was followed by a surge in sterile inflammation and a transient hypopyon, highlighting the delicate balance between infection control and inflammation suppression in these eyes.
Corneal perforation may be managed with cyanoacrylate glue and a BCL as a temporising measure. Progression to descemetocele and recurrent leaks often requires tectonic surgery. Where the ocular surface can be stabilised, PK offers structural rehabilitation and a chance of visual improvement, although persistent epithelial defects and neovascularisation carry high risks of graft failure. In end-stage disease, alternatives such as conjunctival (Gundersen) flaps may prioritise comfort over vision [3–5].
Conclusion
Stevens–Johnson syndrome can produce relentless ocular morbidity despite early and comprehensive care. This case underscores three priorities: (1) urgent ophthalmic involvement with surface protection and epithelial rescue; (2) proactive adnexal management – including lash control and eyelid / tear conservation procedures – to minimise blink trauma and desiccation; and (3) staged escalation from temporising measures (AMT, glue, BCL) to definitive reconstruction (tectonic grafts/PK) once the surface is sufficiently quiet. Even with best practice, chronic complications and limited visual outcomes are common; nonetheless, coordinated, timely interventions can preserve the globe, reduce pain and improve quality of life.
References
1. Duong TA, Valeyrie Allanore L, Wolkenstein P, Chosidow O. Severe cutaneous adverse reactions to drugs. Lancet 2017;390:1996–2011.
2. Letko E, Papaliodis DN, Papaliodis GN, et al. Stevens–Johnson syndrome and toxic epidermal necrolysis: a review of the literature. Ann Allergy Asthma Immunol 2005;94:419–36.
3. Kohanim S, Palioura S, Saeed HN, et al. Acute and chronic ophthalmic involvement in Stevens–Johnson syndrome/toxic epidermal necrolysis—a comprehensive review and guide to therapy. II. Ophthalmic disease. Ocul Surf 2016;14:168–88.
4. Iyer G, Srinivasan B, Agarwal S, et al. Comprehensive approach to ocular consequences of Stevens–Johnson syndrome—the aftermath of a systemic condition. Graefes Arch Clin Exp Ophthalmol 2014;252:457–67.
5. Iyer G, Srinivasan B, Agarwal S. Ocular sequelae of Stevens–Johnson syndrome: a comprehensive approach. Cornea 2020;39(Suppl):S3–S6.
Declaration of competing interests: None declared.



