With two million people in the UK living with visual impairment [1], being able to provide equitable and effective communication to this group of patients is essential in primary care. Yet, as highlighted by research conducted by Sight Loss Councils, 9/10 people living with blindness are denied accessible communication from their healthcare provider [2].
According to the Department of Health’s NHS Next Stage Review Final Report, the NHS is required to give patients autonomy over their own health, through providing easy-to-understand information and ‘good communication’ [3]. In response to patients being routinely sent written communication from their general practice (GP) surgeries in normal-sized font, we sought to optimise written communication to address individual accessibility needs. A literature review on PubMed using terms related to visual impairment, primary care and written communication did not yield any studies evaluating GP correspondence with sight-impaired patients. However, we did note the Macular Society’s guidance on ‘Preparing documents for visually impaired people’ [4].
Aim and method
To ensure 100% of patients at GP surgeries who are registered as blind or partially sighted receive paper communications with appropriately sized fonts to optimise their ability to read them. The project aimed to improve accessibility, enhance communication and improve patient experience across all GP surgeries.
We used the ‘Model for Improvement’ approach as the basis for our quality improvement project (QIP). We first interrogated four GPs’ electronic patient record (EPR) systems to establish how many patients were registered as blind or partially sighted. Most EPRs have filters accessible via the ‘Practice Manager’ which facilitate effortless identification of such patient groups.
Audit
An audit of the visually impaired population was undertaken to establish who would be eligible for the QIP. The QIP population was identified from patient records and each received a telephone call from one of the authors who conducted a questionnaire interview. The questionnaire assessed the following parameters:
- Whether blind or partially sighted (information from patient records, confirmed verbally by patient)
- Patient self-reported level of reading disability
- Format of communication they habitually receive from their GP (electronic or paper)
- How the patient reads their communication (family or friend, visual aids such as magnifiers, text-to-speech, etc.)
- Exclusion factors:
a. Cognitive impairment
b. Limited English proficiency
c. Patients who receive electronic communications
d. Unwillingness to adapt to life withoutvisual aids.
Friends or family who are nominated communication assistants of patients were also contacted to ensure patients were given the best chance to benefit from the QIP.
Intervention 1
A letter in font size 25 was posted to the patient immediately following the telephone interview. The letter thanked the patient for their participation in the QIP and presented them with a range of font sizes (20 to 60) further down for them to choose from. The largest font size of 60 was chosen as it was the upper limit of what appeared reasonable on an A4 letter. Patients were notified during the telephone interview and in the letter that a follow-up telephone call would occur one week after the intervention.
Intervention 1 follow-up
A second telephone-call questionnaire took place one week after Intervention 1. The second questionnaire established the patient’s preferred font size from the range provided. This follow-up also gave the patient the opportunity to offer suggestions as to how they would like their letter font style and format personalised. Suggestions included removing colours (black and white), bold font and double spacing. Patients who were unable to read Intervention 1 themselves were excluded from Intervention 2.
Intervention 2
A letter in the patient’s preferred font size, font style and formatting was posted on the same day immediately after Intervention 1 follow-up. The letter thanked the patient for their continued participation in the QIP and assured them that future communications would be in their preferred font size unless the patient stated any further changes were required. Patients were notified that a follow-up telephone call would occur one week after Intervention 2.
Intervention 2 follow-up
A third telephone-call questionnaire took place a week after Intervention 2. The third questionnaire established which aspects of personalisation the patient preferred.
Implementation
To ensure each patient’s preferred font size and personalisation were included in future physical communications from their GP, these details were added to the patient’s EPR home page which is visible to any administrative staff who send letters to the patient. In each participating site, the same study design was followed as summarised in Figure 1.
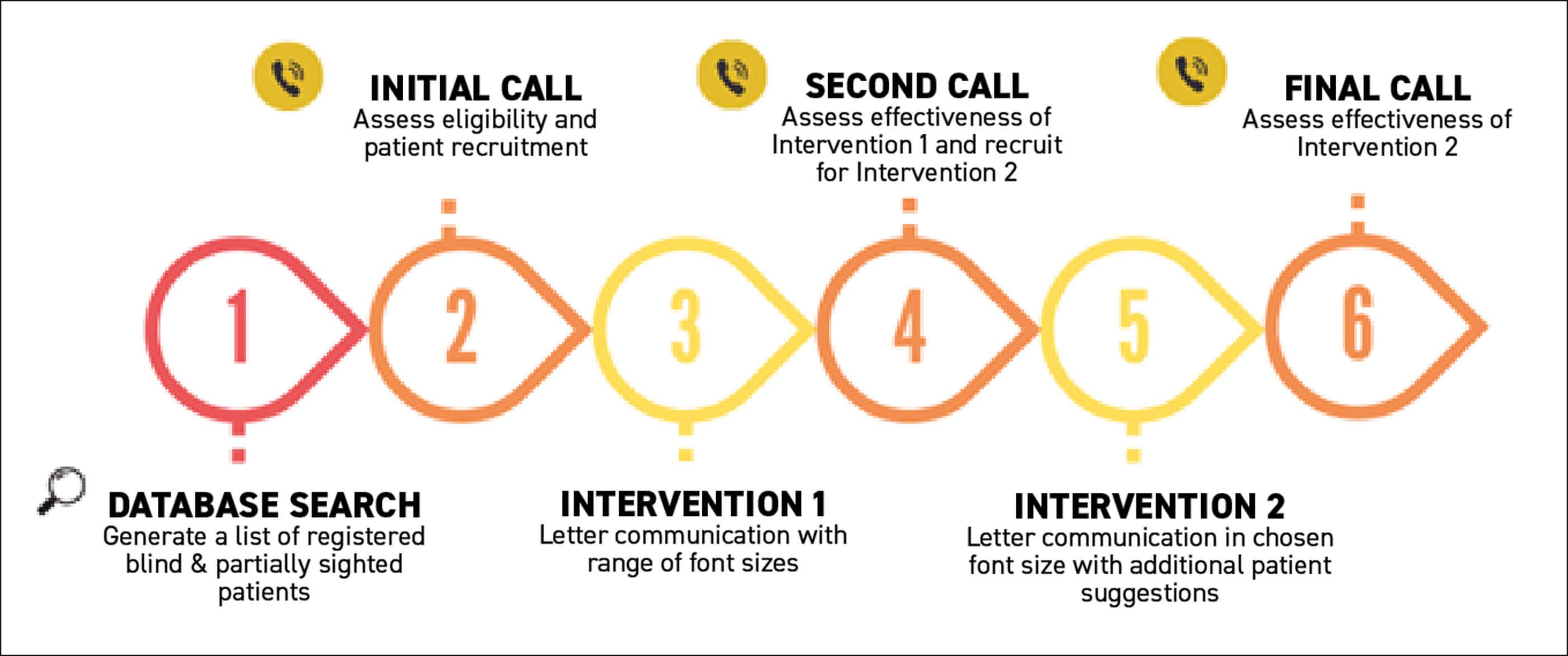
Figure 1: Study design.
Results
Across the four participating GP surgeries, 51 patients were identified as being registered blind or partially sighted. Of these, 35 patients (68.63%) were excluded at the initial assessment stage, most commonly due to factors such as communication being managed by carers, patient preference for electronic communication, cognitive impairment, or feeling that larger-print correspondence would not offer additional benefit to them.
A total of 16 patients (31.37%) proceeded to Intervention 1. Across these 16 patients, four (25.00%) were lost to follow-up or became ineligible after Intervention 1, leaving 12 patients able to proceed to Intervention 2. Before completion of the final follow-up assessment, one further patient (8.33%) was lost, resulting in 11 of the 16 intervention-eligible patients (68.75%) completing the full intervention pathway.
Among the 11 patients who completed Intervention 2, the preferred font sizes ranged from size 30 to size 60. The most commonly selected sizes were 30, 35, 45 and 55, each chosen by two patients, while font sizes 40, 50, and 60 were selected by one patient each (Figure 2).
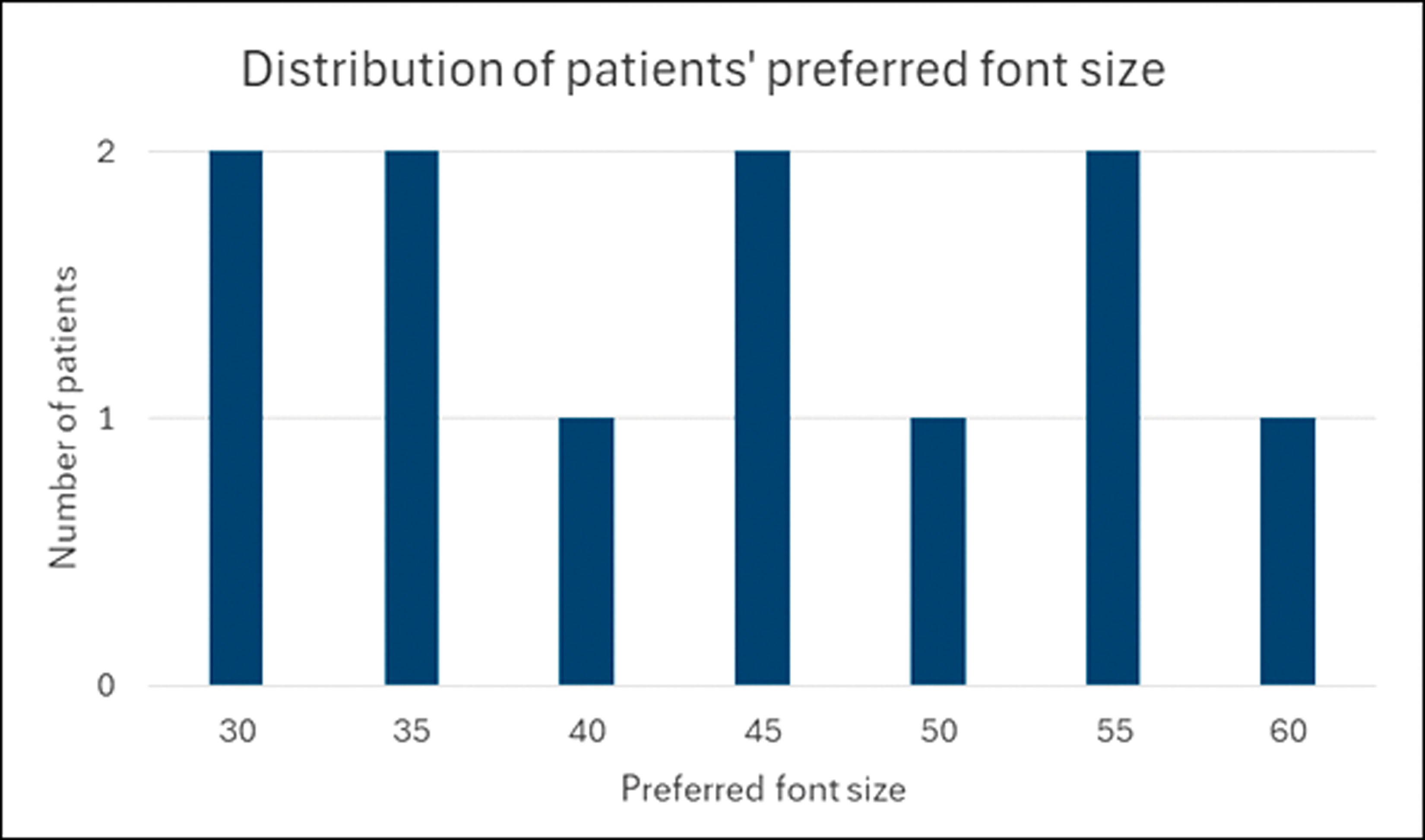
Figure 2: Distribution of patients’ preferred font size.
Discussion
Our QIP employed a co-production approach – working directly with our patients to identify tailored interventions which addressed their individual needs. Personalised interventions were crucial due to the ambiguity of the terms blind or partially sighted and whilst there are medical definitions for these terms, discussion with patients identified them as having varying levels of sight. This contact gave us valuable insight into the experiences of visually impaired patients.
Whilst our initial audit focused on all registered patients coded as blind or partially sighted following a formal ophthalmological assessment/diagnosis, we noted the potential that we may have excluded those patients who had not been formally assessed/diagnosed but still experienced some form of visual impairment. To address this, the practices could introduce simple prompts for patients (or those caring for them) who would prefer their written communications to be in a larger font and/or differently formatted to share this information with their practices. This could include physical large font signs within the practices themselves and perhaps inclusion of text advising this on existing written communications. Importantly, patients with cognitive decline preventing them from being able to read written communications need to be catered for regardless of their visual impairment.
The broad distribution of preferred font sizes demonstrates that there was no single optimum font size that met the needs of all visually impaired patients. The variation showed the importance of individualised tailoring, as even within a relatively small cohort, preferences spanned more than a 30-point range. This finding reinforces the aim of the audit, that standardised written communication in primary care is unlikely to be accessible for many visually impaired patients and that bespoke formatting is essential to improve readability and patient engagement.
Moving forward, to ensure these patients can continue to independently read practice letters, we have placed a notification on each of their EPR home screens including their preferred font size and tailored font formatting requirements and have encouraged them to contact the practice if there are any changes to their vision.
Conclusion
This project has demonstrated that simple changes to written communication such as increasing font size, emboldening text, increasing spacing between lines and black and white formatting can enable patients registered as blind or partially sighted to take more control of and be more actively involved in their healthcare. As a result, 78.57% (11/14) patients with cognitive ability who were previously reliant on a third party and/or visual aids to read our communication no longer needed these.
References
1. www.rnib.org.uk/professionals/
research-and-data/key-information
-and-statistics-on-sight-loss-in-the-uk/
2. www.sightlosscouncils.org.uk/
news/nine-out-of-ten-blind-people
-denied-access-to-health-information/
3. www.gov.uk/government/
publications/high-quality-care-for-all
-nhs-next-stage-review-final-report
4. www.macularsociety.org/
professionals/preparing-documents/
[All links last accessed March 2026]
Declaration of competing interests: None declared.
Acknowledgements:
Birches Medical Centre (East of England), Martlesham Heath Surgery (East of England), Limelight Health and Wellbeing Hub (North West of England) and Sutterton Surgery (East Midlands) for allowing us to access their data; Dr Alicia Jeremiah (Foundation Year 2 Doctor at LLH supporting data collection); Dr Eeman Naeem (Foundation Year 1 Doctor at SS supporting data collection); Mr Nigel Mason (QI Coach); Professor Christopher Liu (Proofreading).








